Listen, if you’ve got a chronic health condition like diabetes, high blood pressure, thyroid disease, or an autoimmune disorder, gettin’ pregnant requires a bit more plannin’ than it does for someone without these issues. But don’t let that discourage you. Millions of women with chronic conditions have healthy pregnancies and healthy babies every single year.
The key is optimization. That means gettin’ your condition under the best possible control before you conceive. When your chronic disease is well-managed, your risk of pregnancy complications drops significantly. When it’s not, well, that’s when problems can happen for both you and your baby.
I’m not gonna sugarcoat it. Pregnancy puts extra stress on your body. Your heart works harder. Your kidneys filter more. Your immune system shifts. Your hormones go crazy. If you’ve already got an organ or system that’s not workin’ perfectly, pregnancy can make those issues worse. But with the right preparation and medical care, you can absolutely have a successful pregnancy.
Why Chronic Disease Management Matters
Here’s the deal. Pregnancy changes everything about how your body functions. Your blood volume increases by almost 50 percent. Your heart rate goes up. Your blood sugar regulation changes. Your immune system has to tolerate a foreign body, your baby, without rejectin’ it. These are massive physiological shifts.
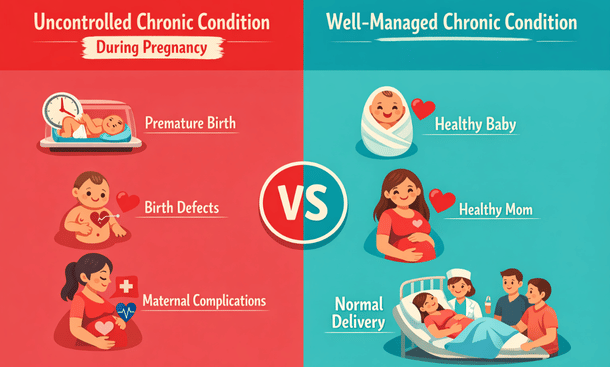
If you have a chronic condition, these pregnancy-related changes can push your body past its comfort zone. Uncontrolled diabetes during pregnancy can cause birth defects and dangerous complications. Unmanaged high blood pressure can lead to preeclampsia and stroke. Unstable thyroid levels can cause miscarriage and developmental problems.
But here’s the flip side. When your chronic condition is well-controlled before you get pregnant, your risks drop dramatically. We’re not talkin’ about small differences here. We’re talkin’ about goin’ from high risk to near-normal risk in many cases. That’s why preconception optimization is so important.
Your doctors need to evaluate your current treatment plan, adjust medications if necessary, optimize your disease control, and establish baseline health markers. This process takes time, sometimes several months. That’s why you can’t wait until you’re already pregnant to start thinkin’ about this stuff.
Thyroid Disease: The Metabolism Master
Your thyroid might be a tiny gland, but it controls your entire metabolism. When it’s not workin’ right, everything in your body can feel off. And when you’re pregnant? Thyroid problems become even more important because your thyroid hormones are crucial for your baby’s brain development, especially in the first trimester.
There are two main thyroid conditions you need to worry about. Hypothyroidism means your thyroid doesn’t produce enough hormone. You might feel tired, gain weight, feel cold, or have trouble concentratin’. Hyperthyroidism is the opposite. Your thyroid produces too much hormone, which can make you feel anxious, lose weight, have a rapid heartbeat, and feel overheated.
Both conditions can make it harder to get pregnant. Hypothyroidism can interfere with ovulation and increase miscarriage risk. Hyperthyroidism can cause irregular periods and reduce fertility. During pregnancy, uncontrolled thyroid disease increases the risk of preeclampsia, preterm birth, low birth weight, and developmental delays in the baby.
The good news? Thyroid disease is incredibly manageable with medication. If you have hypothyroidism, you take levothyroxine, a synthetic thyroid hormone. If you have hyperthyroidism, you might take medications like propylthiouracil or methimazole to slow down your thyroid. Both conditions require regular blood tests to monitor your levels and adjust your medication dose.
Before you start tryin’ to conceive, your thyroid-stimulating hormone, or TSH, should be between 0.5 and 2.5 mIU/L. This is a tighter range than the normal non-pregnant range because pregnancy increases your thyroid hormone needs. Your doctor will check your TSH and possibly your free T4 levels and adjust your medication until you’re in the optimal range.
Once you’re pregnant, your thyroid medication needs will likely increase. Most women with hypothyroidism need about a 30 to 50 percent increase in their levothyroxine dose during pregnancy. That’s why you’ll have frequent thyroid checks throughout pregnancy to make sure your levels stay where they need to be.
Type 1 and Type 2 Diabetes: Blood Sugar Control
Diabetes is one of the most important conditions to optimize before pregnancy. Uncontrolled blood sugar during the first eight weeks of pregnancy, when your baby’s organs are formin’, significantly increases the risk of birth defects, especially heart defects and neural tube defects. We’re talkin’ about risks that are three to four times higher than in women without diabetes.
High blood sugar during pregnancy also increases your risk of miscarriage, stillbirth, preeclampsia, and havin’ a very large baby, which makes delivery more difficult and increases the chance of C-section. After birth, babies of mothers with poorly controlled diabetes can have low blood sugar, breathin’ problems, and jaundice.
But listen to this. When your blood sugar is well-controlled before conception and throughout pregnancy, your risk of complications is almost the same as women without diabetes. Almost the same. That’s incredible, and it shows just how important preconception optimization is.
Your target hemoglobin A1C before pregnancy should be below 6.5 percent, ideally closer to 6 percent if you can achieve that without frequent low blood sugar episodes. A1C measures your average blood sugar over the past three months, so it gives a good picture of your overall control. You should be checkin’ your A1C every three months in the preconception period.
If you’re not at goal yet, work with your endocrinologist or diabetes educator to tighten up your control. This might mean adjustin’ your insulin doses, changin’ the timing of your medications, using a continuous glucose monitor, or switchin’ to an insulin pump. Some oral diabetes medications aren’t safe during pregnancy, so your doctor might need to switch you to insulin before you conceive.

High Blood Pressure: The Silent Threat
High blood pressure, or hypertension, is called the silent killer because it often doesn’t cause symptoms until it’s caused serious damage. During pregnancy, high blood pressure becomes even more dangerous because it can lead to preeclampsia, a potentially life-threatening condition that affects both you and your baby.
Preeclampsia causes dangerously high blood pressure, protein in the urine, and damage to organs like your liver and kidneys. It can lead to seizures, stroke, placental abruption, and premature delivery. Babies born to mothers with preeclampsia are often small and premature because the placenta doesn’t function properly.
If you have chronic hypertension, meanin’ you had high blood pressure before pregnancy, your risk of developin’ preeclampsia is much higher than someone with normal blood pressure. But when your blood pressure is well-controlled before and during pregnancy, that risk decreases significantly.
Your blood pressure should be below 140/90 before you start tryin’ to conceive. Ideally, it should be closer to 120/80. You’ll need to check your blood pressure regularly at home and keep a log so your doctor can see patterns and adjust your treatment if needed.
Some blood pressure medications aren’t safe during pregnancy. ACE inhibitors and ARBs, which are very common blood pressure drugs, can cause birth defects and kidney problems in babies. If you’re takin’ these medications, your doctor will switch you to safer options like methyldopa, labetalol, or nifedipine before you conceive.
Even if your blood pressure is controlled with lifestyle changes alone, like diet, exercise, and weight management, you’ll need closer monitoring during pregnancy. Pregnancy can cause blood pressure to rise even in women who never had problems before, so havin’ a history of hypertension means you need extra vigilance.
Autoimmune Diseases: When Your Body Attacks Itself
Autoimmune diseases like lupus, rheumatoid arthritis, multiple sclerosis, and inflammatory bowel disease present unique challenges during pregnancy. These conditions cause your immune system to attack your own tissues, and pregnancy’s effect on the immune system can be unpredictable. Some women feel better during pregnancy. Others have flare-ups.
The biggest concern with autoimmune diseases is active disease during conception and early pregnancy. Active lupus, for example, increases the risk of miscarriage, preterm birth, preeclampsia, and blood clots. Active inflammatory bowel disease can lead to poor nutrition and premature delivery. That’s why achievin’ disease remission before pregnancy is critical.
You should be in remission or have low disease activity for at least six months before tryin’ to conceive. This gives your body time to stabilize and reduces the chance of a flare-up during pregnancy. Work closely with your rheumatologist, gastroenterologist, or neurologist to optimize your treatment plan.
Many immunosuppressive medications used to treat autoimmune diseases aren’t safe during pregnancy. Methotrexate, for instance, can cause severe birth defects and must be stopped at least three months before conception. Your doctor will switch you to pregnancy-safe alternatives like hydroxychloroquine for lupus or certolizumab for rheumatoid arthritis.
Some women worry that pregnancy-safe medications won’t control their disease as well as their current drugs. That’s a legitimate concern, but uncontrolled disease during pregnancy is more dangerous than most pregnancy-compatible medications. Your doctor will find the best balance between disease control and fetal safety.
Asthma: Breathing for Two
Asthma affects about 8 percent of pregnant women, makin’ it one of the most common chronic conditions in pregnancy. The good news is that asthma doesn’t usually affect your ability to get pregnant. The concern is keepin’ your asthma controlled during pregnancy so you and your baby get enough oxygen.
Poorly controlled asthma during pregnancy increases the risk of preeclampsia, preterm birth, low birth weight, and C-section. When you have an asthma attack, your oxygen levels drop, which means your baby’s oxygen levels drop too. Severe, prolonged oxygen deprivation can affect fetal growth and development.
About one-third of pregnant women with asthma get better during pregnancy. Another third stay the same. And the final third get worse. There’s no way to predict which group you’ll fall into, so you need to be prepared for any scenario.
Your asthma should be well-controlled before you conceive. That means you’re not usin’ your rescue inhaler more than twice a week, you’re not wakin’ up at night with symptoms, and you’re not limitin’ your activities because of breathin’ problems. If you’re experiencin’ any of these issues, your asthma isn’t optimally controlled.
Most asthma medications are safe during pregnancy, includin’ inhaled corticosteroids and short-acting beta-agonists like albuterol. The benefits of controllin’ your asthma far outweigh any small theoretical risks from medications. Uncontrolled asthma is much more dangerous to your baby than asthma medication.
Work with your pulmonologist or allergist to develop an asthma action plan before pregnancy. This plan should outline your daily medications, how to recognize worsenin’ symptoms, when to use your rescue inhaler, and when to seek emergency care. Keep this plan handy throughout pregnancy and share it with your prenatal care provider.
Epilepsy: Seizure Management
Epilepsy requires careful preconception plannin’ because both uncontrolled seizures and certain anti-seizure medications can harm a developin’ baby. It’s a delicate balance between protectin’ you from seizures and protectin’ your baby from medication side effects.
Seizures during pregnancy, especially generalized tonic-clonic seizures, can cause injury to you and decreased oxygen to your baby. They increase the risk of miscarriage, preterm labor, and placental abruption. So stayin’ seizure-free during pregnancy is critically important.
At the same time, some anti-seizure medications, particularly valproic acid and phenytoin, significantly increase the risk of neural tube defects and other birth defects. If you’re takin’ one of these medications, your neurologist will try to switch you to a safer option like lamotrigine or levetiracetam before you conceive.
The goal is to find the lowest effective dose of the safest medication that keeps you seizure-free. Sometimes this requires tryin’ different medications or combinations before you find the right fit. This process can take several months, which is why you need to start plannin’ well before you want to get pregnant.
All women with epilepsy should take high-dose folic acid, at least 4 to 5 milligrams daily, startin’ before conception. This is much higher than the standard prenatal vitamin dose of 400 to 800 micrograms. High-dose folic acid helps reduce the risk of neural tube defects associated with anti-seizure medications.
Kidney Disease: Filtering for Two
Your kidneys work overtime during pregnancy. They have to filter about 50 percent more blood than usual, which puts significant stress on these vital organs. If you already have chronic kidney disease, this extra workload can be problematic.
The impact of pregnancy on kidney disease depends on how well your kidneys are functionin’ before you conceive. If your kidney function is mildly impaired, with a creatinine level below 1.5 mg/dL, pregnancy usually doesn’t cause permanent damage. But if your kidney function is more severely impaired, pregnancy can accelerate kidney disease progression.
Women with kidney disease have higher risks of preeclampsia, preterm birth, low birth weight, and stillbirth. The worse your kidney function, the higher these risks become. That’s why preconception counselin’ with a nephrologist is essential if you have kidney disease.
Your doctor will check your kidney function with blood tests measurin’ creatinine and estimated glomerular filtration rate, or eGFR. They’ll also check for protein in your urine, which indicates kidney damage. If your kidney function is stable and you don’t have significant protein spillage, pregnancy may be safe with close monitoring.
Some medications used to treat kidney disease and its complications aren’t safe during pregnancy. If you’re takin’ ACE inhibitors or ARBs for kidney protection, you’ll need to switch to alternative medications. Your blood pressure control becomes even more important when you have kidney disease because it helps protect your kidneys from further damage.
Heart Disease: Pumping for Two
Heart disease during pregnancy ranges from minor heart valve abnormalities to serious conditions like congenital heart defects or previous heart attacks. The severity of your heart condition determines how much risk pregnancy poses to you and your baby.
Your heart has to work much harder during pregnancy. Your cardiac output, which is the amount of blood your heart pumps per minute, increases by 30 to 50 percent. For women with heart disease, this extra demand can lead to heart failure, dangerous heart rhythms, or even death in severe cases.
Before you get pregnant, you need a complete cardiac evaluation includin’ an echocardiogram to assess your heart function. Your cardiologist will use this information to counsel you about pregnancy risks and determine whether pregnancy is safe for you.
Some heart conditions carry very high maternal mortality risk and pregnancy is not recommended. These include severe pulmonary hypertension, severe left-sided obstruction, and certain complex congenital heart defects. If you have one of these conditions, your cardiologist will have an honest conversation with you about the risks.
For women with moderate heart disease who can safely become pregnant, close monitoring is essential. You’ll need frequent cardiology visits and possibly adjustments to your heart medications. Some cardiac drugs like warfarin aren’t safe during pregnancy and need to be switched to alternatives like heparin.
Mental Health Conditions: Brain Chemistry and Pregnancy
Depression, anxiety, bipolar disorder, and other mental health conditions require thoughtful preconception plannin’. These aren’t just emotional issues. They’re medical conditions caused by brain chemistry imbalances, and they can significantly impact pregnancy outcomes if left untreated.
Untreated depression during pregnancy increases the risk of preterm birth, low birth weight, and postpartum depression. Untreated bipolar disorder can lead to severe mood episodes that affect your ability to care for yourself and your baby. The risks of untreated mental illness often outweigh the risks of medication.
The conversation around psychiatric medications during pregnancy is complicated because research is limited. We know more about some medications than others. Selective serotonin reuptake inhibitors, or SSRIs, are the most studied antidepressants in pregnancy and most are considered relatively safe, though some carry small risks.
Work with your psychiatrist to review your medications before pregnancy. Some psychiatric drugs, like valproic acid used for bipolar disorder, have known risks and should be avoided. Others, like lithium, require careful monitoring but can be used if necessary. Your doctor will weigh the risks and benefits for your specific situation.
Don’t stop your psychiatric medications cold turkey without medical supervision. Abrupt discontinuation can trigger severe withdrawal symptoms or relapse of your mental illness. If you and your doctor decide to change medications or adjust doses, do it gradually under close supervision.

Serene Self-Care Sanctuary
Weight Management and Metabolic Syndrome
Obesity and metabolic syndrome, which includes high blood pressure, high blood sugar, abnormal cholesterol, and excess abdominal fat, significantly increase pregnancy risks. Women with obesity have higher rates of gestational diabetes, preeclampsia, C-section, and birth defects.
If your BMI is over 30, losin’ even a modest amount of weight before pregnancy can reduce your risks. A 5 to 10 percent weight loss can improve fertility, decrease complications, and make pregnancy and delivery safer. That said, pregnancy is not the time for aggressive weight loss or restrictive dietin’.
Work with your doctor or a registered dietitian to develop a healthy eatin’ plan before pregnancy. Focus on nutrient-dense foods, appropriate portion sizes, and regular physical activity. Avoid crash diets or extreme exercise programs. Slow, steady weight loss is healthier and more sustainable.
Some women consider weight loss surgery before pregnancy. Bariatric surgery can be an excellent option for women with severe obesity who haven’t been successful with other weight loss methods. However, you need to wait at least 12 to 18 months after surgery before gettin’ pregnant to allow your weight to stabilize and avoid nutritional deficiencies.
If you’ve had bariatric surgery in the past, inform your prenatal care provider. You’ll need careful nutritional monitoring during pregnancy because surgery can affect how your body absorbs vitamins and minerals. You might need higher doses of prenatal vitamins and more frequent blood work to check for deficiencies.
Medication Management: What’s Safe and What’s Not
One of the most important aspects of chronic disease management before pregnancy is reviewin’ all your medications. Some drugs that are perfectly safe when you’re not pregnant can cause serious problems for a developin’ baby. Your doctors need to evaluate every single medication and supplement you take.
Medications fall into different pregnancy categories based on their safety profile. Category A drugs have been proven safe in pregnant women. Category X drugs are known to cause birth defects and should never be used during pregnancy. Most drugs fall somewhere in between, with varying levels of risk.
Common medications that need to be stopped or switched before pregnancy include ACE inhibitors and ARBs for blood pressure, statins for cholesterol, methotrexate for autoimmune diseases, isotretinoin for acne, and certain anti-seizure medications. Your doctor will find safer alternatives before you conceive.
Don’t make medication changes on your own. Always consult with your prescribin’ doctor before stoppin’, startin’, or changin’ doses of any medication. Some drugs need to be tapered off slowly to avoid withdrawal or disease flare-ups. Others need to be out of your system for a certain period before conception.
Over-the-counter medications and supplements need to be reviewed too. Some herbal supplements can interfere with your chronic disease treatment or aren’t safe during pregnancy. Even things that seem harmless, like high-dose vitamin A or certain pain relievers, can be problematic.

Collaborative Medication Review
Building Your Medical Team
Managin’ a chronic disease during pregnancy requires a team approach. Your obstetrician or midwife will handle your prenatal care, but they’ll need to work closely with your specialist, whether that’s an endocrinologist, cardiologist, nephrologist, rheumatologist, or psychiatrist.
Before you get pregnant, schedule appointments with all your specialists to discuss your pregnancy plans. They need to communicate with each other to coordinate your care. Ask each specialist to send your obstetrician a summary of your condition, current treatment, and any special considerations for pregnancy.
You might need to see a maternal-fetal medicine specialist, also called a perinatologist, if your chronic condition puts you in the high-risk pregnancy category. These doctors specialize in complicated pregnancies and work alongside your regular OB to provide extra monitoring and care.
Create a binder or digital folder with all your medical records, test results, medication lists, and specialist contact information. Keep this organized and bring it to all your appointments. When multiple doctors are involved in your care, good communication and record-keeping are essential.
Don’t be shy about askin’ questions or advocatin’ for yourself. You know your body better than anyone. If somethin’ doesn’t feel right or you’re not comfortable with a treatment plan, speak up. Your medical team should listen to your concerns and work with you to find solutions.
Monitoring and Follow-Up
Once your chronic condition is optimized and you start tryin’ to conceive, you’ll need continued monitoring to make sure everything stays on track. The frequency of follow-up depends on your specific condition and how stable it is.
Women with diabetes need frequent blood sugar checks and A1C tests. Women with thyroid disease need TSH checks every 6 to 8 weeks in the preconception period and more frequently during pregnancy. Women with high blood pressure need regular blood pressure monitoring at home and in the office.
Keep detailed records of your health metrics. Use apps, spreadsheets, or paper logs to track blood sugars, blood pressure, medication doses, symptoms, and any changes in your condition. This information helps your doctors make informed decisions about your treatment.
When you do get pregnant, notify all your specialists right away, not just your obstetrician. Your medication needs might change immediately. For example, thyroid medication usually needs to be increased as soon as pregnancy is confirmed. Your specialists need to know so they can adjust your treatment promptly.
Living with Chronic Disease and Planning Pregnancy
Havin’ a chronic health condition doesn’t mean you can’t have a baby. It just means you need to be more intentional and strategic about your plannin’. With proper optimization, close monitoring, and good medical care, most women with chronic diseases have successful pregnancies and healthy babies.
The preconception period is your opportunity to get everything in the best possible shape. Use this time wisely. Work closely with your medical team. Make lifestyle changes that support your health. Get your medications optimized. And give yourself grace when things don’t go perfectly.
Remember that preconception optimization isn’t just about lab values and medications. It’s also about stress management, adequate sleep, good nutrition, regular exercise, and emotional wellbeing. All these factors affect your chronic disease control and your overall health.
Optimizing chronic health conditions before pregnancy is one of the most important steps you can take to protect both your health and your baby’s health. From thyroid disease and diabetes to autoimmune disorders and heart conditions, proper management significantly reduces pregnancy risks and improves outcomes.
You’ve already completed important preconception health screenings including STI and immunity testing to protect against infections. Now you’ve learned how to optimize existing health conditions to create the safest possible environment for pregnancy.
Don’t forget that preconception health isn’t just about you. Your partner’s health matters too. Learn about male preconception health tests and screening to ensure both of you are in optimal health before starting your family.
For a comprehensive overview of all recommended preconception medical assessments, from basic blood work and hormone testing to STI screening, chronic disease optimization, and partner health evaluations, return to our complete guide to preconception health tests. It provides the complete roadmap for preparing both partners for a healthy pregnancy.