
Breastfeeding is one of those things everyone tells you is natural, but nobody warns you about the actual challenges that come with it. You’re sitting there at two in the morning with cracked nipples, a screaming baby who won’t latch, and breasts that feel like rocks, wondering what the hell you’re doing wrong. The truth is, you’re probably not doing anything wrong at all. Most new moms run into at least one major breastfeeding problem in those early weeks, and some deal with multiple issues at once.
I’ve been there, and I’ve talked to hundreds of moms who’ve been there too. Sore nipples, clogged ducts, low supply anxiety, babies who refuse the breast—these aren’t signs that breastfeeding isn’t for you. They’re normal complications that have real solutions once you understand what’s happening and what actually works to fix it.
This guide walks you through the most common breastfeeding problems you’re likely to encounter, from minor annoyances to situations that need medical attention. More importantly, it gives you practical, no-BS solutions that actually work instead of vague reassurances that everything will magically get better. Some problems resolve in a day or two with the right approach. Others take more time and effort. Either way, you deserve to know what you’re dealing with and what your options are.
Breastfeeding doesn’t have to be painful or constantly stressful. Once you get past the initial learning curve and handle whatever specific issues come up for you, most moms find it becomes significantly easier and more comfortable. But getting to that point requires addressing problems head-on instead of trying to tough it out and hoping they disappear on their own.
Sore nipples and pain during breastfeeding
Nipple pain is probably the number one complaint from new breastfeeding moms, and it’s also the most common reason women stop nursing earlier than they planned. If your nipples are sore, cracked, or bleeding, every feeding session becomes something you dread instead of a bonding experience with your baby.
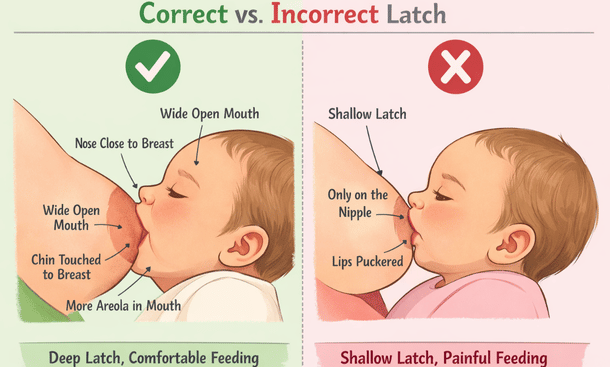
The vast majority of nipple pain comes from a poor latch. When your baby doesn’t take enough breast tissue into their mouth and latches onto just the nipple, it creates friction and pressure that damages your skin. A proper latch should include a good portion of your areola, not just the nipple tip. Your baby’s mouth should be wide open, their lips flanged outward, and you should see more areola visible above their top lip than below their bottom lip.
Positioning plays a huge role in whether your baby can achieve a good latch. If you’re hunched over, holding your baby at an awkward angle, or not bringing them in close enough to your body, they can’t latch deeply no matter how hard they try. Your baby should be tummy-to-tummy with you, with their head tilted back slightly so their chin touches your breast first.
Beyond latch problems, thrush is another common cause of nipple pain. This yeast infection creates intense burning pain that doesn’t go away between feedings. You might notice shiny or flaky skin on your nipples, and your baby might have white patches in their mouth. Thrush requires antifungal treatment for both you and your baby.
For immediate relief while you work on fixing the underlying cause, medical-grade lanolin creates a protective barrier over damaged skin. Hydrogel pads provide cooling relief and speed up healing. Your own breast milk rubbed onto your nipples after feeding has antibacterial properties that help repair damaged tissue. Air drying your nipples completely between feedings prevents moisture from slowing down the healing process.
Getting a lactation consultant to watch you nurse can identify latch issues you might not see yourself. Sometimes it’s a tiny adjustment in how you hold your baby or position your breast that makes all the difference. Many hospitals offer free lactation support in those first few weeks.
Physical issues like tongue tie or lip tie can make it impossible for your baby to latch deeply no matter what you try. These are restrictions in the tissue under your baby’s tongue or upper lip that prevent proper mouth movement. A pediatrician or lactation consultant can diagnose these conditions, and they’re usually fixed with a quick procedure.
Most nipple pain improves dramatically within three to five days once you correct the latch and use proper aftercare. If you’ve got persistent cracks that won’t heal, fever, or intense burning pain shooting into your breast, you need medical attention because these could indicate infection or thrush. Our complete guide on how to fix sore nipples while breastfeeding fast walks you through relief strategies and latch correction techniques in detail.
Low milk supply and increasing production
Worrying about whether you’re making enough milk is one of the biggest sources of stress for breastfeeding moms. The anxiety is real, but here’s something important to understand. Most moms who think they have low supply are actually producing plenty of milk. Perceived low supply is way more common than actual low supply.
Your body operates on a supply and demand system. The more your breasts get emptied, the more milk they make. Every time your baby nurses or you pump, it sends signals to your brain to produce prolactin, which creates milk, and oxytocin, which releases it. The frequency and thoroughness of breast emptying directly determines how much milk your body produces.
Babies nurse constantly in the early weeks because they’re programming your body to make the right amount for them. They go through growth spurts where they suddenly want to eat all the time. They cluster feed in the evenings. They nurse for comfort, not just food. None of this means you don’t have enough milk. It means your baby is doing exactly what they’re supposed to do.
Real low supply shows up as poor weight gain, fewer than six wet diapers a day after the first week, dark concentrated urine, or a baby who seems genuinely hungry and unsatisfied after long nursing sessions. If your baby is gaining weight appropriately and producing plenty of wet diapers, you almost certainly have adequate supply even if it doesn’t feel like it.
For moms who genuinely need to boost production, the solution comes down to removing milk more frequently and more thoroughly. Nurse every two to three hours during the day and at least once or twice at night. Power pumping, where you pump for twenty minutes, rest for ten, pump for ten, rest for ten, then pump for ten more once a day, mimics cluster feeding and can jump-start production.
Making sure your baby is actually draining your breasts effectively matters more than how often they nurse. A poor latch or tongue tie means your baby might nurse constantly without removing much milk. If your breasts still feel full after nursing, that’s a red flag worth investigating with a lactation consultant.
Staying hydrated and well-fed supports milk production. You need an extra three hundred to five hundred calories a day while breastfeeding, and cutting calories to lose weight can tank your supply. Drink water every time you nurse and don’t skip meals.
Galactagogues like oats, fenugreek, and blessed thistle have some evidence for boosting supply, though results vary between individuals. Prescription medications like domperidone can increase prolactin levels but come with potential side effects and are typically reserved for moms who’ve tried everything else.
Most interventions take three to five days before you notice a difference, sometimes up to two weeks to reach full effect. Track your baby’s output and weight gain instead of obsessing over how many ounces you pump. Many moms don’t respond well to pumps even when they have plenty of milk for direct nursing.
Engorgement and clogged milk ducts
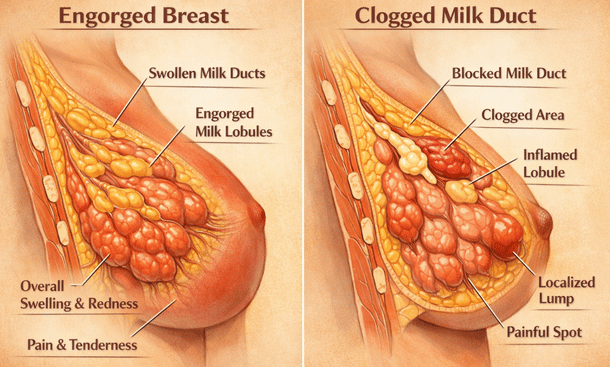
Engorgement and clogged ducts both make your breasts feel hard and painful, but they’re different problems that need different approaches. Understanding which one you’re dealing with helps you treat it effectively before it turns into something worse.
Engorgement usually hits in the first week or two after birth when your milk first comes in. Your entire breast suddenly gets massively full, tight, hot, and painful. The whole breast is affected, not just one spot. Your skin might look shiny and stretched, and you might even run a low-grade fever. This happens because your body is still figuring out how much milk to make, so it overproduces initially. Engorgement typically affects both breasts equally.
A clogged duct is a localized blockage in one specific milk duct. You’ll feel a distinct hard lump or tender spot in one area of your breast while the rest feels fine. The skin over the clogged area might look red or feel warm. Clogged ducts usually happen in just one breast at a time, though you can get unlucky and deal with both. They’re often triggered by pressure on the breast from a tight bra, sleeping on your stomach, a heavy bag strap, or going too long between feedings.
For clogged ducts, time matters because the longer a duct stays blocked, the more likely it is to get infected. Heat is your first move. Apply a warm compress or heating pad to the affected area for ten to fifteen minutes before nursing to help dilate the ducts and get things flowing. Standing in a hot shower and massaging the lump works great too.
Massage while you nurse, using firm but gentle pressure to work the lump toward your nipple in long strokes. Position your baby so their chin points toward the clogged area because gravity and their sucking pressure work together to drain that specific duct. This might mean trying weird positions like nursing on all fours with your baby underneath you if the clog is on top of your breast.
Dangle feeding, where you lean over your baby on all fours while they nurse lying on their back, uses gravity to help pull the milk down and out. It looks ridiculous but it’s surprisingly effective for stubborn clogs. After nursing, use cold compresses to reduce inflammation and pain.
Keep nursing frequently on the affected side even though it hurts. You need to keep emptying that breast. If your baby won’t nurse enough or the lump isn’t budging, pump after feedings to make sure you’re fully draining the breast. A vibrating massager or electric toothbrush applied directly to the clog while nursing can help break it up.
Lecithin supplements, one two hundred milligram capsule three to four times a day, make your milk less sticky so it flows more easily through ducts. This works better as prevention for recurrent clogs than as immediate treatment for an active blockage.
For engorgement, nursing frequently every one to two hours is the most important thing you can do. Your body needs to get the message to slow down production, and that only happens when milk gets removed regularly. If your breast is so hard that your baby can’t latch, hand express or pump just enough to soften the areola first. This is called reverse pressure softening.
Cold cabbage leaves tucked inside your bra for about twenty minutes provide relief for some women, but don’t overdo it because excessive use can decrease your supply. Cold compresses between feedings help reduce swelling and pain. Wear a supportive but not tight bra with no underwires.
Anti-inflammatory medication like ibuprofen is safe while breastfeeding and helps with both pain and swelling from either engorgement or clogged ducts. Take it as directed instead of trying to tough out the discomfort.
Both conditions can progress to mastitis if left untreated, so you need to know the warning signs. Fever over one hundred point four degrees, red streaks spreading from the affected area, and flu-like symptoms mean the inflammation is getting worse and you need medical attention. If your symptoms aren’t improving after twenty-four hours of aggressive home treatment, call your doctor.
Prevention is easier than treatment. Nurse on a consistent schedule, avoid tight bras and pressure on your breasts, don’t sleep on your stomach, stay hydrated, and gradually wean when you’re ready instead of dropping feedings suddenly. If you’re prone to recurrent clogs, daily lecithin can make a real difference. You can find detailed relief techniques and prevention strategies in our guide on clogged milk duct relief that actually works fast.
Mastitis and breast infections
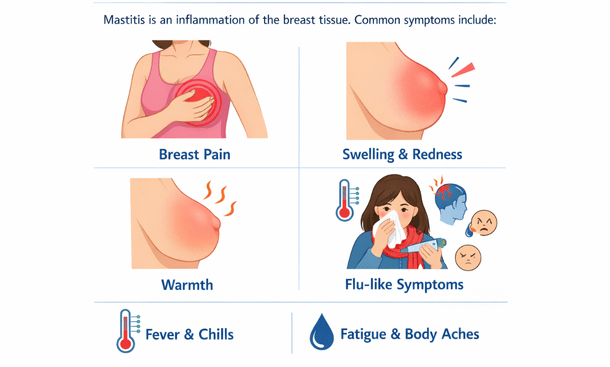
Mastitis is not something you wait out or try to handle on your own without medical guidance. This is a breast infection that needs immediate attention because it can escalate quickly from uncomfortable to seriously problematic. If you’ve got a fever, a red painful area on your breast, and you feel like you’ve been hit by a truck, you’re likely dealing with mastitis.
Mastitis happens when bacteria get into your breast tissue through a cracked nipple or when a clogged duct doesn’t clear and the backed-up milk creates an environment where bacteria can multiply. The most common bacteria involved is Staphylococcus aureus, which normally lives on everyone’s skin but causes problems when it gets where it shouldn’t be. Sometimes mastitis is just severe inflammation from a badly clogged duct without actual bacterial infection, but you can’t always tell the difference without medical evaluation.
The symptoms come on strong and fast. Fever is the hallmark sign, often spiking to one hundred point four degrees or higher, sometimes reaching one hundred and three. You’ll get chills, body aches, exhaustion, and headache that feel exactly like the flu. Your affected breast will be red, often with a wedge-shaped area of redness or red streaks spreading outward. The skin feels hot compared to your other breast, and the pain ranges from a deep ache to sharp stabbing sensations.
The infected area feels firm and swollen. Some women notice their milk looks different, maybe stringy or containing pus, though this isn’t always visible and your milk is usually still safe for your baby even when it looks weird. You might feel a hard lump that won’t drain even after nursing, which was probably the original clogged duct that started everything.
The key difference between mastitis and a simple clogged duct is those systemic symptoms. If you’ve got fever and feel sick all over your body, not just breast pain, that’s mastitis and you need to call your doctor immediately.
Don’t wait to see if it gets better overnight. Call your healthcare provider as soon as you suspect mastitis. Most providers will prescribe antibiotics without needing to see you if your symptoms are clear, though some want you to come in for evaluation. The most common prescriptions are dicloxacillin or cephalexin for ten to fourteen days. You must take the full course even after you start feeling better, otherwise the infection can come back stronger and potentially become resistant to treatment.
Keep nursing or pumping despite the pain. This sounds counterintuitive when your breast is killing you, but continuing to empty the breast is crucial for healing. The milk is safe for your baby because the infection is in your tissue, not in the milk itself. If you stop nursing, the breast stays full, the infection worsens, and you risk developing an abscess, which is a pocket of pus that requires drainage.
Nurse frequently on the affected side, every two hours if you can manage it. Start each feeding on the infected breast so your baby drains it when their suck is strongest. If nursing is too painful, pump instead, but don’t let the breast stay full.
Rest is not optional with mastitis. Your body is fighting an infection and needs energy to do that. Get someone to help with the baby between feedings, sleep when the baby sleeps, and cancel everything non-essential. Trying to power through and maintain your normal schedule will just make recovery take longer.
Stay hydrated with water, juice, or whatever fluids sound good. Take ibuprofen regularly for pain and inflammation, not just when it gets unbearable. Apply heat before nursing to help with letdown and milk flow, and use cold compresses between feedings to reduce inflammation.
You should start feeling significantly better within twenty-four to forty-eight hours of starting antibiotics. If you’re not improving after two days on antibiotics, call your doctor back. You might need a different antibiotic or there could be an abscess forming that needs drainage.
An abscess is a pocket of pus in the breast tissue that develops when mastitis isn’t clearing up properly. If you feel a distinct fluid-filled lump that’s getting bigger despite treatment, you need to be seen. Abscesses usually require drainage with a needle or minor surgery, but you can still continue breastfeeding afterward.
Recurring mastitis suggests an underlying problem worth investigating. Maybe your baby has a tongue tie affecting their latch, or you’ve got an oversupply issue, or there’s resistant bacteria involved. Work with both a lactation consultant and your doctor to figure out why it keeps happening.
Prevention focuses on treating clogged ducts immediately before they progress, not going too long between feedings, avoiding tight bras and pressure on your breasts, taking care of cracked nipples right away since they’re entry points for bacteria, and managing stress and exhaustion as much as possible since these lower your immune system.
Some women find that taking probiotics regularly helps prevent recurrence by supporting immune function and maintaining healthy bacteria balance. Basic hygiene like washing your hands before nursing and keeping pumping equipment clean also matters when you’ve got broken skin on your nipples.
Breastfeeding through mastitis absolutely sucks, but stopping will make it worse and take longer to heal. The pain during nursing usually gets somewhat better after initial letdown once milk is flowing. Try different positions to find what hurts least, with side-lying often being more comfortable than sitting up.
Your milk supply might temporarily drop while you’re sick, but it’ll come back once you recover if you keep nursing frequently. Your baby won’t get sick from nursing while you have mastitis, and the antibiotics you’re taking are safe for breastfeeding.
If you’re not feeling significantly better after forty-eight hours on antibiotics, if your fever goes away but comes back after a few days, if the red area is spreading instead of shrinking, or if you’re feeling worse instead of better, don’t wait to follow up. Go to urgent care or the emergency room if you can’t reach your regular doctor. Our comprehensive guide on mastitis symptoms and treatment walks through recognition, treatment options, and when to escalate care in more detail.
Baby won’t latch or refuses the breast
Few breastfeeding problems are more frustrating than a baby who simply won’t latch onto your breast. You’re sitting there with breasts full of milk, a hungry crying baby, and no matter what you try, they either refuse to latch or latch so poorly that nobody’s happy. This situation can make you feel like you’re failing at something that’s supposed to be natural, but latching problems are incredibly common and most have solutions once you identify what’s actually going on.
Babies refuse the breast or struggle to latch for a bunch of different reasons, and sometimes it’s a combination of factors working against you. Understanding the cause makes it way easier to fix the problem instead of just trying random things and hoping something works.
Tongue tie or lip tie are physical restrictions where the tissue under your baby’s tongue or upper lip is too tight. This prevents them from opening their mouth wide enough or moving their tongue properly to create a good latch. They might try to nurse but slip off repeatedly, make clicking sounds, or seem to work really hard without getting much milk. You might notice your baby can’t stick their tongue out past their bottom lip or their tongue looks heart-shaped when they cry.
Flat or inverted nipples make it harder for babies to latch because there’s less for them to grab onto. Your baby needs to take in a good amount of areola, not just nipple, and if your nipple doesn’t protrude much, they struggle to get a deep latch going. The good news is nipples often become more protractile after a few weeks of nursing as your baby’s sucking literally helps draw them out over time.
Nipple confusion happens when babies get bottles or pacifiers early on and then prefer the different sucking motion or faster flow. They get frustrated at the breast because it requires more work and the milk doesn’t come as quickly. Strong letdown or fast flow can overwhelm a baby, especially a newborn, causing them to pull off, sputter, cough, or refuse to latch because they can’t handle the spray.
Slow letdown or low supply creates the opposite problem where your baby latches, sucks a few times, doesn’t get immediate reward, and gives up in frustration. Positioning and technique issues are probably the most common cause of latching problems overall. If you’re not holding your baby at the right angle, not supporting their head properly, or not getting their mouth wide enough before they latch, it’s not gonna work well no matter how much you both try.
Pain from a previous difficult feeding can make babies develop an aversion. If latching hurt them before because of a bad latch or fast flow, they might remember that and resist trying again. Nursing strikes can happen at any age where a baby who previously nursed fine suddenly refuses, usually triggered by things like teething, ear infections, changes in routine, or stress. These are almost always temporary.
Skin-to-skin contact is magic for encouraging latching. Strip your baby down to just a diaper, take off your shirt and bra, and hold them against your bare chest. This triggers their feeding instincts and helps them naturally root and find the breast. Spend at least twenty to thirty minutes doing this before you even try to actively get them to latch.
Wait for a wide open mouth before attempting to latch. Don’t try to shove your nipple into a partially open mouth. Tickle your baby’s lips with your nipple until they open really wide, like a yawn. Then bring them quickly onto your breast, aiming your nipple toward the roof of their mouth. Their bottom lip should be far below your nipple with more areola visible above their top lip than below their bottom lip.
The cross-cradle hold gives you the most control over your baby’s head and makes it easier to guide them onto the breast. The football hold works well if you’ve had a c-section or if your baby arches away in the cradle hold. Side-lying is good for relaxed practice sessions, and laid-back or biological nursing positions let gravity help while allowing your baby to use their natural reflexes.
Breast shaping or the nipple sandwich technique works great if you’ve got larger breasts or a smaller baby. Compress your breast from top and bottom so it’s flatter, like a sandwich, which makes it easier for your baby to get a big mouthful. Express a little milk first to soften the areola if you’re engorged and to give your baby an immediate taste of milk as motivation.
If you suspect tongue or lip tie, you need evaluation by someone trained to spot these issues. Not all pediatricians recognize them, so you might need to see a lactation consultant, pediatric dentist, or ENT specialist. If a tie is confirmed, the treatment is a simple procedure called a frenotomy where they clip or laser the restrictive tissue. It takes seconds, causes minimal discomfort, and your baby can nurse immediately after.
Nipple shields can be a helpful temporary tool for flat or inverted nipples. These thin silicone covers go over your nipple and give your baby something more prominent to latch onto. They’re not a long-term solution because they can reduce milk transfer, but they can get you through the early weeks while your baby gets stronger.
For babies with bottle preference, you need to stop or minimize bottle use if possible and use paced bottle feeding when you do give bottles. This means holding the bottle horizontal, letting your baby control the flow, and taking breaks during feeding to make it more similar to breastfeeding in terms of effort. Offer the breast when your baby is calm and alert, not starving, and try offering during drowsy times when they’re less likely to protest.
Most nursing strikes last three to five days. Keep offering the breast without pressure, maintain your supply by pumping, and give lots of skin-to-skin contact. Try offering when your baby is very sleepy, in the bath, while walking around, or in different positions and locations. Feed your baby pumped milk by cup, syringe, or spoon rather than bottle if possible to avoid reinforcing bottle preference.
Get help from a lactation consultant if you’ve tried everything and your baby still won’t latch, if nursing is extremely painful despite different techniques, or if your baby isn’t gaining weight properly. They can observe a full feeding, spot issues you’re missing, and give you personalized strategies. Join a breastfeeding support group where hearing that other moms dealt with the same thing and got through it helps enormously.
Latching problems are frustrating as hell, but most improve with time, practice, and the right support. Babies get bigger and stronger, their mouths grow, they get more coordinated. What’s impossible at two days old often becomes easy at two weeks old. It’s okay to use tools like shields or supplemental nursing systems if that’s what keeps your baby fed while you work through the issues. For detailed troubleshooting techniques and position guidance, our guide on tried-and-true ways to get your baby to breastfeed covers latch strategies comprehensively.

Breastfeeding problems are normal, not a sign that you’re failing or that nursing isn’t meant for you. Every single issue we’ve covered in this guide, from sore nipples to mastitis to babies who won’t latch, happens to thousands of moms every day. You’re not alone in dealing with this stuff, and more importantly, you’re not stuck with it.
The biggest mistake moms make is trying to tough it out and hoping problems will resolve on their own. Some issues do get better with time as you and your baby figure things out together. But others, like clogged ducts or cracked nipples, get worse when you wait instead of taking action. The faster you address problems, the faster you get relief and the lower your risk of complications.
Nine times out of ten, breastfeeding challenges come down to latch and positioning. If you take nothing else from this guide, remember that a proper deep latch solves or prevents most common problems. Your baby’s mouth needs to cover a good portion of your areola, not just clamp down on your nipple. Their body should be pulled in close to yours, tummy-to-tummy, with their head tilted back slightly. Getting this right makes everything else easier.
Don’t be afraid to ask for help. Lactation consultants exist specifically to help you troubleshoot these problems, and most hospitals offer free support in those first few weeks. Your pediatrician, your OB, online support groups, local breastfeeding meetups—all of these are resources you can and should use when you’re struggling. Nobody gets a medal for suffering through breastfeeding problems alone.
Know when to get medical attention. Fever, red streaks, severe pain that’s getting worse instead of better, or a baby who’s not gaining weight properly all require professional evaluation. Trust your gut when something feels wrong. It’s always better to check in with your doctor and have it be nothing than to let a treatable problem become a serious complication.
Also know that it’s okay to change course if breastfeeding isn’t working for you despite your best efforts. Some moms deal with anatomical issues or medical conditions that make exclusive breastfeeding extremely difficult or impossible. Some babies have challenges that can’t be fully resolved. Fed is best, whether that’s exclusive breastfeeding, combo feeding with formula, exclusively pumping, or formula feeding. Your mental health and your baby’s wellbeing matter more than any feeding method.
For most moms though, breastfeeding does get easier after those first few challenging weeks. Once you and your baby figure out your rhythm, fix whatever specific problems came up, and get past the initial learning curve, nursing usually becomes comfortable and even enjoyable. You just have to get through the rough patch first, and that’s where knowing what you’re dealing with and what actually works to fix it makes all the difference.
Take things one feeding at a time, one problem at a time. You don’t have to solve everything at once. Address whatever’s causing you the most pain or stress right now, get that under control, then move on to the next thing if needed. Small improvements add up quickly.
Remember that your experience is valid regardless of how it compares to other moms. Some women sail through breastfeeding with zero problems. Others deal with multiple complications. Neither experience is more legitimate than the other, and struggling doesn’t mean you’re doing something wrong. It just means you hit some bumps in the road that need addressing.
Stay patient with yourself and your baby. You’re both learning, and learning anything new comes with frustration and setbacks. The fact that you’re reading this guide and looking for solutions shows you’re committed to making breastfeeding work, and that determination matters more than anything else.
If you’re dealing with painful, cracked nipples right now and need immediate relief while you work on fixing your latch, start with our detailed guide on how to fix sore nipples while breastfeeding fast. It covers everything from lanolin and hydrogel pads to proper latch technique and when to suspect tongue tie. Getting comfortable again makes everything else easier to handle.
You’ve got this. Breastfeeding problems suck, but they’re temporary and solvable. Keep asking questions, keep trying solutions, and don’t give up on yourself.

As a Felyro.com content author, I develop actionable content on breastfeeding, translating research-backed information into practical advice for mothers. My goal is to help families establish healthy feeding habits, improve maternal confidence, and support infant development.