
Listen, I’m not gonna sugarcoat this for you. Finding out you have a high-risk pregnancy is scary as hell.
One minute you’re excited about being pregnant, maybe planning the nursery or thinking about names. The next minute your doctor is using words like “complications” and “specialist referral” and suddenly everything feels different. Heavier. More fragile.
I get it because I’ve been there. At 33 years old with what I thought was a perfectly healthy pregnancy, I got slapped with the high-risk label at my 20-week ultrasound. Just like that, everything changed. More appointments. More tests. More worry.
But here’s what I learned through my own experience and through years of working with women navigating complicated pregnancies. High-risk doesn’t mean hopeless. It doesn’t mean your pregnancy is doomed or that something terrible will definitely happen.
What it actually means is that you need extra attention, closer monitoring, and specialized care to give you and your baby the best possible outcome. Modern medicine has come incredibly far in managing pregnancy complications. Things that would have been catastrophic 30 years ago are now totally treatable with the right medical team and the right information.
That’s what this guide is really about. Giving you the information you need to understand what’s happening, what to expect, and how to advocate for yourself throughout this journey. Because knowledge is power when you’re dealing with medical uncertainty.
You’re not alone in this. About 6-8% of pregnancies in the United States are considered high-risk, which means hundreds of thousands of women go through this every year. Most of them deliver healthy babies and come out the other side okay.
This isn’t the pregnancy you imagined, but it’s still your pregnancy. You can still have moments of joy and connection with your baby even while dealing with medical complications. You can still prepare for motherhood even when things feel uncertain.
Let’s walk through everything you need to know about high-risk pregnancy care, from understanding your diagnosis to managing complications to taking care of yourself along the way.
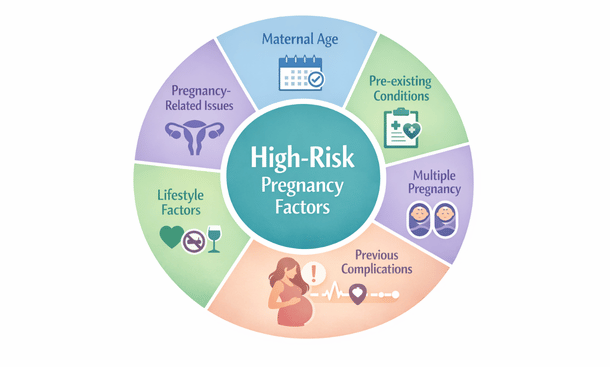
Understanding What Makes a Pregnancy High-Risk
The term “high-risk pregnancy” gets thrown around a lot but what does it actually mean?
In medical terms, it simply indicates an increased chance of complications for you or your baby during pregnancy, labor, or delivery. That increased chance could be small or significant depending on your specific situation. Some women are barely above baseline risk while others need serious medical intervention.
Your age plays a bigger role than most people want to admit. If you’re under 17 or over 35, you’re automatically considered at higher risk. I know that sounds harsh, especially for those of us who waited until our thirties to start families. But the statistics don’t lie.
Younger moms face risks related to their bodies not being fully developed for pregnancy. Teen pregnancies have higher rates of preterm birth and low birth weight babies. For those of us over 35, being of “advanced maternal age” means increased chances of chromosomal abnormalities, gestational diabetes, preeclampsia, and placenta previa.
Pre-existing medical conditions are probably the biggest category that lands women in the high-risk zone. If you walked into pregnancy already managing diabetes, high blood pressure, thyroid disease, autoimmune disorders, kidney disease, or heart conditions, you’re gonna need specialized care throughout your pregnancy.
The pregnancy itself can create complications even if you started out healthy. Carrying multiples automatically makes you high-risk. Previous pregnancy complications like preeclampsia, gestational diabetes, or preterm labor mean you’re more likely to experience those same issues again.
Lifestyle factors matter too, though nobody likes to talk about this part. Smoking, alcohol use, drug use, being significantly overweight or underweight all raise your risk level. These aren’t moral judgments, just medical realities that affect pregnancy outcomes.
Sometimes multiple risk factors combine to create a higher-risk situation. Maybe you’re 38 years old with well-controlled hypothyroidism carrying twins. Each factor individually raises your risk, and together they require even closer monitoring.
The key thing to understand is that being labeled high-risk means you need more medical attention than someone with an uncomplicated pregnancy. You’ll see your doctor more often. You’ll have more tests and ultrasounds. You might work with maternal-fetal medicine specialists in addition to your regular OB-GYN.
But all that extra attention is actually good news. Problems get caught early when they’re easier to treat. Your medical team has the information they need to make good decisions about your care. The surveillance might feel overwhelming but it exists to protect you and your baby.
Different risk factors require different approaches to care. Someone with well-controlled diabetes will have a different care plan than someone dealing with placenta previa. Your specific situation determines what tests you need, how often you’re monitored, and what precautions matter most.
Understanding exactly what puts you in the high-risk category helps you know what to watch for and what questions to ask your medical team. It puts you in a position of knowledge rather than just passively hoping everything works out.
The classification isn’t permanent either. Sometimes risk factors resolve or improve as pregnancy progresses. A low-lying placenta diagnosed at 20 weeks might move up and away from the cervix by 32 weeks, eliminating that particular concern. Other times new complications develop and the level of risk increases.
Your care plan should evolve based on how your pregnancy is actually going, not just based on your initial risk assessment. This is why regular monitoring matters so much. Your medical team needs current information to make informed decisions.
Working with specialists who understand high-risk pregnancy makes a huge difference in outcomes. Maternal-fetal medicine doctors have additional training specifically in managing complicated pregnancies. They see these situations every day and know how to handle them.
Don’t be afraid to ask why you’re considered high-risk and what that means specifically for you. Some doctors use the term pretty loosely while others reserve it for more serious situations. Get clarity on your particular risk factors and what the actual concerns are.
Knowledge about your classification empowers you to be an active participant in your care rather than just a patient things are happening to. You can make informed decisions, ask relevant questions, and advocate for yourself effectively when you understand what you’re dealing with.
Recognizing Warning Signs That Need Immediate Attention
One of the most important things you can do during a high-risk pregnancy is learn to recognize which symptoms require immediate medical attention.
Normal pregnancy comes with all sorts of weird aches, pains, and discomforts. Your body is literally growing another human and everything gets stretched, compressed, and rearranged in the process. But when you’re high-risk, your margin for error is smaller. What might be no big deal for someone with an uncomplicated pregnancy could signal a serious problem for you.
Heavy bleeding is never something to brush off. Some light spotting can be normal, especially in early pregnancy. But if you’re soaking through a pad in an hour or less, that’s a problem. Bright red blood that looks like a heavy period needs immediate attention. This could indicate placental abruption or other serious complications that require emergency care.
Severe abdominal pain that doesn’t go away when you change positions or rest is different from normal pregnancy discomfort. Round ligament pain is sharp and brief, usually triggered by movement. But constant, intense pain could signal something serious like appendicitis, kidney infection, or placental problems.
Headaches during pregnancy are common thanks to hormonal changes and stress. But severe headaches that don’t respond to rest or acetaminophen are a different story, especially if they come on suddenly and feel unlike any headache you’ve had before. Combined with vision changes like seeing spots or blurred vision, this is one of the hallmark symptoms of preeclampsia.
Vision problems on their own warrant immediate evaluation. Seeing flashing lights, having tunnel vision, or experiencing sudden blurriness isn’t normal pregnancy stuff. These symptoms can indicate dangerously high blood pressure affecting your eyes and brain.
Sudden, severe swelling especially in your face and hands is concerning. Some swelling in your feet and ankles is totally normal by the end of the day or in your third trimester. But if you wake up one morning and your face is puffy and your rings won’t come off when they fit fine yesterday, that’s a red flag for preeclampsia.
Decreased fetal movement requires immediate attention once you’re past the point where you feel regular movement. You know your baby’s patterns better than anyone else. If something feels off or you’re not feeling your normal amount of activity, call your doctor or go to labor and delivery to get checked.
Shortness of breath that’s severe or sudden is not normal even in late pregnancy when your uterus is squashing your lungs. If you can’t catch your breath even when sitting still, or if breathing becomes painful, you could be dealing with a pulmonary embolism or heart problem.
Signs of preterm labor before 37 weeks need evaluation right away. Regular contractions that get progressively stronger and closer together, pelvic pressure like the baby is pushing down, lower back pain that comes and goes, or your water breaking all warrant immediate medical attention.
Fever over 100.4°F during pregnancy always needs to be reported to your doctor. It can indicate infection, and some infections are particularly dangerous during pregnancy. Combined with other symptoms like severe abdominal pain or chills, fever becomes even more concerning.
The most important thing I can tell you about recognizing these warning signs is to trust your instincts. You know your body better than anyone else. If something feels wrong even if you can’t articulate exactly what’s different, that instinct is worth listening to.
I’ve talked to so many women who said they just knew something was off before they even had obvious symptoms. Every single one of them wished they’d called their doctor sooner instead of talking themselves out of it because they didn’t want to seem paranoid.
Your medical team would much rather you call about a false alarm than ignore a real problem. That’s literally what they’re there for. You’re not bothering them. You’re not overreacting. You’re advocating for yourself and your baby.
Keep your doctor’s after-hours number handy. Know where your nearest emergency room is and how to get there quickly. Have a plan for childcare or pet care if you have to go to the hospital unexpectedly.
Not every concerning symptom requires an emergency room visit, but some absolutely do. Call your doctor’s office first for things like decreased fetal movement, mild bleeding or spotting, or persistent headache. They’ll tell you whether you need to come in right away or if it can wait.
Go directly to the emergency room for heavy bleeding, severe abdominal pain, chest pain or severe difficulty breathing, sudden severe headache with vision changes, signs of preterm labor, your water breaking, or any symptom that just feels like an emergency.
When in doubt, err on the side of caution. The worst that happens is they check you out and send you home. The best that happens is they catch something serious before it becomes critical. Understanding which symptoms demand immediate action gives you the power to protect yourself and your baby when it matters most.
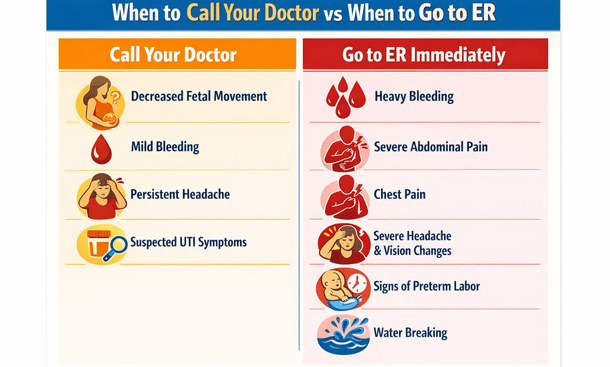
Medical Decision Guide
Essential Medical Testing and Monitoring
Get ready to become very familiar with medical offices and testing facilities if you haven’t already.
In a normal pregnancy, you typically get two or maybe three ultrasounds total. In a high-risk pregnancy, you might get one every few weeks or even weekly depending on what’s being monitored. The frequency of appointments and testing depends on your specific situation, but expect to be seen a lot more than women with uncomplicated pregnancies.
First trimester screening usually kicks things off for high-risk pregnancies, especially if you’re over 35 or have a family history of genetic conditions. The combined screening happens between 11 and 14 weeks and involves a blood test measuring two proteins plus an ultrasound measuring the fluid at the back of your baby’s neck.
Cell-free DNA testing, also called NIPT, has become increasingly popular because it’s more accurate than traditional screening. They just draw your blood and analyze tiny fragments of your baby’s DNA floating around in your bloodstream. The test screens for chromosomal conditions and can tell you your baby’s sex super early if you want to know.
If screening results show increased risk, your doctor will probably recommend definitive testing like CVS or amniocentesis. These tests involve actually taking a sample from inside your uterus, which sounds terrifying but provides definitive answers about genetic conditions.
CVS happens earlier at 10-13 weeks and involves collecting a tiny sample of placental tissue. Amniocentesis happens later, typically between 15-20 weeks, and involves withdrawing a small amount of amniotic fluid. Both carry a small risk of miscarriage, usually quoted around 0.1-0.3%, but doctors have gotten really good at these procedures with modern ultrasound guidance.
The anatomy scan around 18-22 weeks is standard for everyone, but high-risk pregnancies often get additional detailed ultrasounds. They check all of your baby’s organs and structures to make sure everything is developing normally. For high-risk situations, you’ll probably get targeted ultrasounds focusing on specific concerns throughout your pregnancy.
Growth scans later in pregnancy track whether your baby is growing appropriately. Babies that are too small or too large both come with risks. The measurements help your doctor decide if and when intervention might be needed. You might get these every 2-4 weeks in the third trimester depending on your situation.
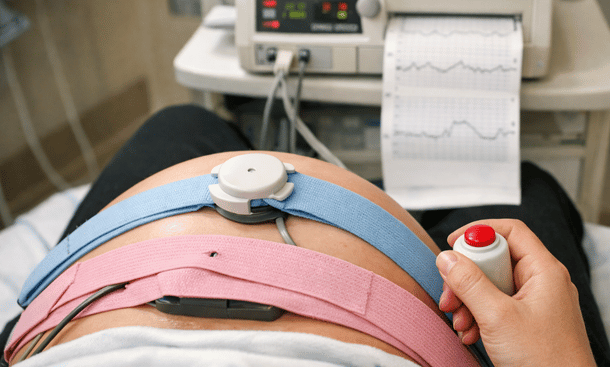
Non-stress tests become a regular thing for many high-risk pregnancies once you hit the third trimester. You basically sit in a recliner for 20-40 minutes while they monitor your baby’s heart rate and any contractions you might be having. What they’re looking for is whether your baby’s heart rate increases when they move, which indicates a healthy, well-oxygenated baby.
I did non-stress tests twice a week for the last month of my pregnancy. It got tedious sitting there for an hour each time, but I also found it weirdly reassuring. Hearing that steady heartbeat and seeing those little accelerations when the baby moved helped calm my anxiety between appointments.
The biophysical profile is a specialized ultrasound that assesses your baby’s wellbeing by looking at movement, muscle tone, breathing practice, and amniotic fluid levels. Combined with a non-stress test, it gives a comprehensive picture of how your baby is doing.
Blood pressure monitoring becomes constant if you’re at risk for preeclampsia. They’ll check it at every single appointment, often multiple times during each visit. You might be asked to monitor it at home between appointments with specific instructions about what numbers should prompt a call to the office.
Urine tests at every visit check for protein, which is a sign of preeclampsia. If they’re worried about it, they might order a 24-hour urine collection where you collect all your urine for 24 hours in a big jug. It’s inconvenient and kind of gross, but it gives the most accurate measurement of protein levels.
Glucose tolerance testing screens for gestational diabetes. Every pregnant woman gets the one-hour test, but high-risk pregnancies often get tested earlier and sometimes more than once. If you fail the one-hour test, you have to do the three-hour glucose tolerance test, which is honestly miserable but necessary.
Specialized blood tests go beyond standard prenatal bloodwork. If you have a clotting disorder, thyroid disease, autoimmune conditions, or other health issues, you’ll get regular blood work to monitor those conditions and make sure any medications you’re taking are at the right dose.
Fetal echocardiography is a specialized ultrasound of your baby’s heart done by a pediatric cardiologist. Not everyone needs this, but it’s common if you have diabetes, a family history of heart defects, or if something looked concerning on a routine ultrasound.
The appointment takes longer than a regular ultrasound, usually 45 minutes to an hour, because the specialist needs detailed views of the heart from multiple angles. They’re checking for congenital heart defects, which are the most common type of birth defect.
Understanding what these tests actually measure and why they matter helps transform them from scary unknowns into useful tools that give your care team information to make good decisions. Each test serves a real purpose in monitoring you and your baby.
Don’t leave appointments confused about results. Ask your doctor to explain what the numbers mean and whether they’re seeing anything concerning. Sometimes results that sound scary are actually totally fine in context.
Keep a dedicated pregnancy binder or folder with all your test results, appointment summaries, and important phone numbers. When you’re juggling multiple providers and seeing doctors multiple times a week, having everything organized in one place becomes essential.
Prepare questions before each appointment and write them down because pregnancy brain is real and you will forget what you wanted to ask. Bring snacks and water, especially for longer appointments. You might be there a while.
The constant testing takes a mental and emotional toll that doesn’t get talked about enough. Some women develop serious anxiety around appointments, constantly waiting for someone to find something wrong. Others become almost numb to it all, just going through the motions.
Try to celebrate the good appointments and good test results instead of just moving immediately to worrying about the next one. Your baby had a great non-stress test? That’s genuinely good news worth acknowledging.
All these tests and monitoring appointments exist to help you have the healthiest pregnancy possible. They’re not punishment or unnecessary medicalization. They’re tools that provide crucial information for managing your care effectively throughout your pregnancy journey.
Managing Complications and Treatment Options
Getting diagnosed with a pregnancy complication is one of those moments that stops time and changes everything about how your pregnancy feels.
Suddenly words like preeclampsia or gestational diabetes or placenta previa become part of your daily vocabulary. Your whole pregnancy shifts from excited anticipation to careful medical management. It’s scary and overwhelming and completely normal to feel thrown off balance by it.
But here’s what I learned through managing my own complications and working with dozens of women through theirs. Most pregnancy complications, even serious ones, are manageable with proper treatment and close monitoring. The key is understanding what’s actually happening and what your options are.
Preeclampsia is probably the complication that scares women the most, and for good reason. It affects roughly 5-8% of pregnancies and is characterized by high blood pressure and usually protein in your urine after 20 weeks. The tricky thing is that it can develop gradually or come on suddenly.
Treatment for preeclampsia depends entirely on severity and how far along you are. Mild preeclampsia before 37 weeks usually means close monitoring with frequent blood pressure checks at home and at the office, regular blood tests to check your liver enzymes and kidney function, and non-stress tests to make sure your baby is doing okay.
Severe preeclampsia is a different story. Blood pressure consistently over 160/110, significant protein in urine, or symptoms like severe headaches and vision changes mean you need immediate treatment, usually in the hospital. Magnesium sulfate prevents seizures, which is the progression to eclampsia that can be fatal.
The only real cure for preeclampsia is delivery. If you’re at or near term, your doctor will probably recommend inducing labor. If you’re very preterm, they’ll try to manage the condition as long as it’s safe for both you and your baby, possibly giving you steroid shots to help your baby’s lungs mature faster.
Gestational diabetes develops when your body can’t produce enough insulin to handle the increased blood sugar demands of pregnancy. It affects about 6-9% of pregnancies and first line treatment is always diet and exercise.
You’ll meet with a nutritionist who’ll teach you about counting carbohydrates and making food choices that keep your blood sugar stable. Eating smaller, more frequent meals throughout the day helps. Pairing carbohydrates with protein slows sugar absorption. Choosing complex carbs over simple sugars makes a real difference.
You’ll check your blood sugar multiple times a day with a glucose meter, usually fasting when you wake up and then one or two hours after each meal. Keeping a food and blood sugar log helps you identify which foods cause spikes and which ones keep you in range.
For many women, diet and exercise manage gestational diabetes through the rest of pregnancy. But somewhere around 10-20% need medication because lifestyle changes alone aren’t cutting it. Insulin is the most common option since it doesn’t cross the placenta. Some doctors use oral medications like metformin instead.
With good management, most women with gestational diabetes have healthy babies. You’ll get extra ultrasounds to monitor growth and non-stress tests in the third trimester to make sure everything is going well.
Placenta previa happens when the placenta covers part or all of the cervix. It’s usually discovered on an ultrasound in the second trimester, and the main symptom is bright red bleeding without pain. Many cases diagnosed early resolve on their own as the uterus grows and the placenta moves away from the cervix.
Treatment depends on severity and how far along you are. If you have previa and start bleeding, you’ll probably be put on pelvic rest, which means no sex, nothing in the vagina, no heavy lifting or strenuous exercise. Severe bleeding might mean hospitalization and bed rest.
The big issue with previa is that you can’t deliver vaginally if the placenta is still covering the cervix at the end of pregnancy. You’ll have a scheduled C-section, usually around 36-37 weeks before you go into labor on your own.
Placental abruption is when the placenta separates from the uterine wall before delivery, which can deprive your baby of oxygen and cause serious bleeding for you. The classic symptoms are severe abdominal pain that doesn’t go away and a hard or tender uterus.
Small abruptions might be managed with bed rest and close monitoring if you’re not close to term and the baby seems okay. But significant abruption usually means emergency delivery regardless of how far along you are because the risks are too high.
Preterm labor is regular contractions that cause your cervix to dilate before 37 weeks. If you’re in early preterm labor and less than 34 weeks, the goal is to stop it if possible. Tocolytic medications can slow or stop contractions temporarily, buying crucial time to give you steroid injections that help your baby’s lungs mature faster.
Two shots of betamethasone 24 hours apart can dramatically improve outcomes for premature babies. It reduces the risk of respiratory distress syndrome, bleeding in the brain, and other complications of prematurity.
Bed rest is often prescribed for preterm labor, though the evidence on its effectiveness is questionable. Progesterone supplementation through vaginal suppositories or weekly injections can help keep the uterus quiet and reduce preterm birth risk.
Cervical cerclage is a surgical option if you have cervical insufficiency, meaning your cervix starts opening too early without contractions. They literally stitch your cervix closed and remove the stitch around 36-37 weeks. It’s usually done between 12-14 weeks if you have a history of second trimester losses.
Intrauterine growth restriction means your baby is measuring smaller than expected and isn’t getting adequate nutrients or oxygen. Management depends on the severity and what’s causing it. You’ll get frequent growth scans to track whether your baby is still growing even if they’re small.
Treatment focuses on addressing underlying causes if possible. Controlling your blood pressure if that’s the issue. Treating infections. Managing other health conditions optimally. The difficult decision comes when tests show the baby is no longer doing well inside and early delivery might be safer than continuing the pregnancy.
Medication safety during complicated pregnancies is a common concern. Low-dose aspirin is commonly prescribed for women at risk of preeclampsia. Blood pressure medications like labetalol and nifedipine are safe during pregnancy. Insulin for diabetes doesn’t cross the placenta. Blood thinners like heparin are necessary for clotting disorders.
The key is weighing risks versus benefits. Untreated high blood pressure or uncontrolled diabetes or untreated clotting disorders are far more dangerous to your baby than the medications used to treat them.
Working with maternal-fetal medicine specialists becomes crucial when complications arise. These are OB-GYNs with additional training in high-risk pregnancies who work alongside your regular OB to manage your care.
Don’t be afraid to ask questions and advocate for yourself. Get copies of all your test results and keep them organized. Build a good relationship with your MFM team because these are the people who will guide you through the scary parts.
The hardest part about complications is the uncertainty. Sometimes treatments work perfectly and you make it to term. Sometimes despite doing everything right, your baby comes early or needs intervention. What matters is that you’re getting the best medical care possible and doing everything you can to protect yourself and your baby.
Understanding your treatment options empowers you to make informed decisions rather than just passively accepting whatever your doctor recommends. You have the right to ask why they’re suggesting a particular approach, what the alternatives are, and what the risks and benefits of each option look like for your specific situation.
Lifestyle Adjustments and Self-Care for High-Risk Mothers
Managing a high-risk pregnancy isn’t just about following doctor’s orders and showing up for appointments. It’s about taking care of yourself day-to-day while dealing with restrictions, uncertainty, and a level of medical surveillance that can feel overwhelming.
The reality is that your whole life changes when you’re labeled high-risk. Maybe you had to quit your job or go on leave. Maybe you’re on bed rest or restricted activity. Maybe you’re just constantly anxious about whether your baby is okay. All of that takes a toll that goes way beyond the physical aspects of pregnancy.
Nutrition becomes more complex when every food choice feels critical. The basic principles of good pregnancy nutrition still apply, but your specific situation might require modifications. If you have gestational diabetes, you’re counting carbs and pairing them with protein to keep your blood sugar stable.
Focus on foods that give you the most nutritional value. Eggs are fantastic with lots of protein and healthy fats. Greek yogurt without added sugar. Nuts and nut butters. Lean meats and fish that are low in mercury. Load up on non-starchy vegetables that are full of vitamins and fiber.
For those dealing with preeclampsia or high blood pressure, reducing sodium matters. That means cooking at home more because restaurant food and processed foods are loaded with salt. Staying hydrated is crucial too because dehydration can trigger contractions and make everything worse.
If you’re on bed rest, you’re burning fewer calories than when you were active. It’s easy to gain excessive weight lying around all day, which can complicate things further. Small frequent meals throughout the day work better than three large meals for most high-risk situations.
Exercise and movement become complicated questions that depend entirely on your specific situation. If you have placenta previa or are at risk for preterm labor, your doctor might say no exercise at all. If you have well-controlled gestational diabetes and no other complications, exercise might be encouraged.
You need specific guidance from your doctor about what’s safe. Don’t assume anything is okay without asking. For most high-risk pregnancies, gentle movement is better than complete inactivity unless you’re on strict bed rest.
Walking is usually safe and beneficial. Even just 10-15 minutes after meals can help with blood sugar control and reduce swelling. Prenatal yoga can be great if your doctor approves it. The stretching and breathing exercises help with stress management and the modified poses are designed for pregnant bodies.
Swimming and water aerobics are low-impact options that take pressure off your joints and feel amazing when you’re carrying around extra weight. What you definitely need to avoid is anything with risk of falling, activities that spike your heart rate too high, or heavy weightlifting.
If you were super active before pregnancy and now you’re limited, the mental adjustment is brutal. You feel like your body is betraying you. You miss the endorphin rush and the sense of accomplishment. Focus on what you can do rather than what you can’t.
Managing stress when everything feels stressful is one of the biggest challenges. High-risk pregnancy is inherently anxiety-provoking. You’re worried about your baby constantly. You’re dealing with medical appointments and tests and uncertainty. Maybe you’re on restricted activity or had to stop working.
Therapy is one of the best investments you can make. Find a therapist who specializes in pregnancy and perinatal mental health. They understand the unique challenges and can give you actual coping strategies. Some therapists do video sessions which is perfect if you’re on bed rest.
Mindfulness and meditation can help even if you’ve never done it before. There are tons of apps with guided meditations specifically for pregnancy. Even just five or ten minutes a day of focused breathing can lower your stress hormones.
I was skeptical about meditation until I was lying in a hospital bed having a panic attack about whether my baby would survive. A nurse taught me a simple breathing technique that didn’t fix everything but gave me something to focus on besides the fear.
Connection with other women going through similar situations makes a huge difference. Online support groups for high-risk pregnancy can be lifesavers, especially if you’re isolated on bed rest. Knowing you’re not alone in this really helps.
Sleep quality often goes to hell during complicated pregnancies. You’re uncomfortable. You’re worried. You have to pee constantly. Your mind won’t shut off. Creating a bedtime routine helps signal to your body that it’s time to sleep.
Sleep on your side, preferably your left side, after the first trimester. This position optimizes blood flow to your baby. A pregnancy pillow makes a huge difference by supporting your whole body. If you don’t want to invest in one, regular pillows work too.
Naps are not a sign of laziness when you’re dealing with pregnancy complications. If you’re exhausted, rest. Your body is working incredibly hard right now and sometimes you just need more sleep.
Figuring out how to handle work when you’re high-risk is complicated and depends entirely on your specific situation and job. Some women can work normally with minor modifications. Others need to cut back hours or switch to desk duty. Some end up on complete leave.
If your doctor puts you on restricted activity or bed rest, you need a note documenting the medical necessity. This protects you under pregnancy discrimination laws and may qualify you for short-term disability or FMLA.
The financial stress of not being able to work is real and doesn’t get talked about enough. You might have to dip into savings or rely on your partner’s income. If working isn’t possible, try to let go of guilt about it. You’re following medical advice to protect your baby.
Building your support system becomes essential because you cannot do this alone. Your partner needs to step up in major ways. They might need to take on more household responsibilities, come to medical appointments, and provide emotional support when you’re scared.
Family support is invaluable if you have it, though family can also be overwhelming with unwanted advice. Set boundaries with people who aren’t helpful. Friends often want to help but don’t know how. Be specific about what would actually be useful.
Hiring help if you can afford it is worth considering. A house cleaner every couple weeks. Grocery delivery service. Meal prep service. These things cost money but they can significantly reduce your stress.
Self-advocacy in medical settings is huge and something I wish I’d understood earlier. You have the right to ask questions and get clear answers. If your doctor uses medical jargon you don’t understand, ask them to explain it in plain English.
Don’t let anyone dismiss your concerns. If something feels wrong or you’re having symptoms that worry you, insist on being evaluated. Trust your instincts about your body. If you’re not comfortable with your care team, get a second opinion or switch providers.
Bring a list of questions to appointments and write them down because pregnancy brain is real. Take notes during appointments or bring someone with you who can help remember information. Ask for copies of all your test results and keep them organized.
Staying connected to your baby can be hard when you’re so focused on complications and risks. But finding small ways to connect helps you remember why you’re going through all this. Talking or singing to your baby creates connection. Feeling your baby move and kick is reassuring.
Looking at ultrasound pictures and imagining what your baby will be like helps make them feel real. Planning for after delivery, even in small ways, can give you something positive to focus on. But it’s also okay if you can’t do those things because you’re too scared.
The emotional roller coaster is real and doesn’t get talked about enough. You’re going to have days where you feel strong and positive and days where you’re terrified and can’t stop crying. Both are normal. You’re dealing with intense medical stress, hormones, physical discomfort, and massive life changes all at once.
Anxiety is incredibly common in high-risk pregnancies. Depression can happen too. If you’re experiencing symptoms like feeling hopeless or losing interest in things you normally enjoy, please talk to your doctor. Prenatal depression is real and treatable.
Grief over the pregnancy experience you’re not having is valid. It’s okay to be sad that your pregnancy isn’t what you imagined. You can grieve that loss while still doing what you need to do. Anger is normal too. It’s not fair that some women sail through pregnancy while you’re dealing with all this.
Let yourself feel whatever you’re feeling without judgment. You don’t have to be grateful and positive all the time. Sometimes things just suck and it’s okay to acknowledge that.
Recovery after a high-risk pregnancy often takes longer than after an uncomplicated pregnancy. Physical recovery from bed rest means rebuilding strength and stamina. Emotional recovery is just as important. Some women experience postpartum PTSD after traumatic high-risk pregnancies.
Give yourself grace as you process everything you went through. Managing a high-risk pregnancy is genuinely hard. You did something difficult and you survived it. That deserves recognition.
Taking care of yourself through all the restrictions and uncertainty isn’t selfish or indulgent. It’s necessary. You can’t take care of your baby if you’re completely burned out and falling apart. Small acts of self-care, realistic expectations about what you can handle, and asking for help when you need it all matter more than you might think during this challenging time.

Look, I’m not gonna stand here and tell you that high-risk pregnancy is easy or that everything will definitely turn out fine if you just stay positive and follow all the rules.
That would be bullshit and you deserve better than platitudes.
The truth is that managing a high-risk pregnancy is hard. It’s scary. It’s exhausting. Some days you’re gonna feel strong and capable and other days you’re gonna cry in the bathroom wondering how you’re supposed to get through the next week, let alone the next few months.
But here’s what I know from my own experience and from walking alongside dozens of women through complicated pregnancies. You’re stronger than you think you are. And you don’t have to do this alone.
The medical advances we have now mean that complications that would have been catastrophic a generation ago are manageable with proper care. Preeclampsia can be monitored and treated. Gestational diabetes can be controlled. Preterm labor can sometimes be stopped or at least delayed long enough to give your baby crucial extra weeks of development.
The key is having the right information, the right medical team, and the right support system around you.
Understanding what makes your pregnancy high-risk gives you knowledge instead of just fear. Recognizing warning signs means you can act quickly when something needs attention. Knowing what tests to expect and why they matter transforms medical surveillance from something scary into something useful.
Managing complications becomes less overwhelming when you understand your treatment options and feel empowered to ask questions and advocate for yourself. And taking care of yourself day-to-day, even within all the restrictions and uncertainty, helps you maintain some quality of life while doing what you need to do to protect your baby.
Your high-risk label doesn’t define your entire pregnancy experience. It’s one part of your story, but not the whole thing. You can still have moments of joy and connection with your baby. You can still prepare for motherhood. You can still look forward to meeting your little one even while dealing with medical complications.
The vast majority of high-risk pregnancies end with healthy moms and healthy babies. The statistics are actually on your side, even though it doesn’t always feel that way when you’re in the thick of it.
Every appointment you show up for matters. Every test you do provides information. Every precaution you take is protecting you and your baby. None of it is meaningless even when it feels overwhelming.
Build your team of specialists and trust them to guide you through the medical aspects. But also trust yourself. You know your body. You know when something feels off. You know what you can handle and what you need help with.
Don’t be afraid to speak up in medical settings. Don’t be afraid to ask for help from family and friends. Don’t be afraid to prioritize your mental health alongside your physical health.
This journey is temporary even though it feels endless when you’re living it. You will get through this. You will meet your baby. And one day, hopefully sooner rather than later, this will be a chapter you look back on rather than the reality you’re living in.
You’re doing better than you think you are. On the days when you feel like you’re barely holding it together, remember that showing up and doing what needs to be done is enough. You don’t have to be perfect. You don’t have to handle everything gracefully. You just have to keep going.
Take it one day at a time. One appointment at a time. One test at a time. Celebrate the good results and the milestones you hit. Be gentle with yourself on the hard days.
And remember that thousands of women have walked this path before you and made it to the other side with their babies in their arms. You’re not alone in this, even when it feels like it.
If you’re struggling with the daily realities of restricted activity, dietary changes, or the emotional weight of managing complications, know that there are practical strategies that can help you maintain your wellbeing while following medical recommendations. Taking care of yourself isn’t just about following doctor’s orders – it’s about finding ways to stay mentally and physically healthy within whatever limitations you’re dealing with.
You’ve got this. And on the days when you don’t feel like you’ve got this, lean on the people and resources around you who can help carry you through.

Carlene R. Priddy offers strategic advice and practical guidance for governorsbefore, during, and after their mandatesto strengthen governance and public leadership.