Getting hit with a pregnancy complication diagnosis is one of those moments that stops time.
Your doctor says words like preeclampsia or gestational diabetes or placenta previa and suddenly your whole pregnancy feels different. Scarier. More fragile. Like one wrong move could mess everything up.
I’ve been there. I’ve sat in that exam room feeling like the floor just dropped out from under me. And I’ve talked to enough women going through the same thing to know that the fear and uncertainty are completely normal reactions.
But here’s what I learned through my own experience and years of working in pregnancy care. Most complications, even serious ones, are manageable with proper treatment and close monitoring. The key word there is manageable, not curable or preventable or no big deal. Just manageable.
Understanding what’s happening in your body and how to navigate the complexities of high-risk pregnancy care can help you move from panic to empowerment.. You’re not helpless. You have choices and actions you can take.
So let’s walk through the most common high-risk pregnancy complications and talk about what actually works to keep you and your baby as safe as possible.
Preeclampsia: The Complication Everyone Fears
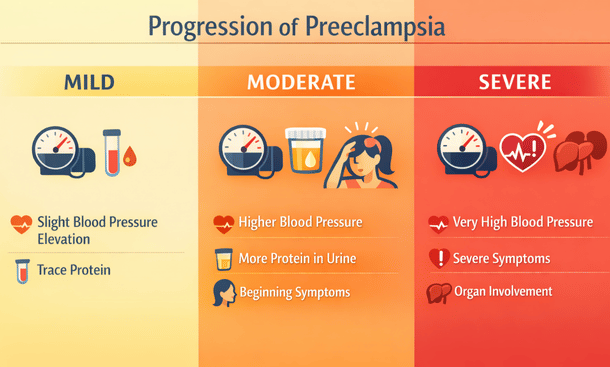
Preeclampsia affects roughly 5-8% of pregnancies and it’s one of the leading causes of maternal and fetal complications worldwide. It’s characterized by high blood pressure and usually protein in your urine after 20 weeks of pregnancy.
The tricky thing about preeclampsia is that it can develop gradually or come on suddenly. Some women have mild symptoms that are manageable for weeks. Others go from normal to severe preeclampsia in a matter of days.
Early warning signs include persistent headaches that don’t respond to acetaminophen, vision changes like seeing spots or blurriness, upper abdominal pain especially under your ribs on the right side, sudden weight gain from fluid retention, and severe swelling in your face and hands.
If your doctor diagnoses preeclampsia, the treatment approach depends on how severe it is and how far along you are in your pregnancy.
Mild preeclampsia before 37 weeks usually means close monitoring. You’ll have frequent blood pressure checks, probably at home and at the doctor’s office. Regular blood tests to check your liver enzymes, kidney function, and platelet count. Urine tests or 24-hour urine collections to monitor protein levels. Non-stress tests to make sure your baby is doing okay.
Some doctors recommend modified bed rest, though the evidence on whether that actually helps is mixed. What definitely helps is reducing stress, staying hydrated, and avoiding strenuous activity.
Severe preeclampsia is a different story. Blood pressure consistently over 160/110, significant protein in urine, abnormal blood work, or symptoms like severe headaches and vision changes mean you need immediate treatment.
You’ll probably be admitted to the hospital for close monitoring and medication to lower your blood pressure. Magnesium sulfate is the standard treatment to prevent seizures, which is the progression to eclampsia that can be fatal.
The only real cure for preeclampsia is delivery. If you’re at or near term, your doctor will probably recommend inducing labor. If you’re very preterm, they’ll try to manage the condition as long as it’s safe for both you and your baby, possibly giving you steroid shots to help your baby’s lungs mature faster in case early delivery becomes necessary.
I developed preeclampsia at 34 weeks. My blood pressure was creeping up for a couple weeks but then it spiked to 170/110 and I had protein in my urine. They admitted me immediately, put me on magnesium sulfate, and delivered my baby at 35 weeks. Those two weeks in the hospital on bed rest with constant monitoring were some of the scariest of my life, but my baby came out healthy and only needed a few days in the NICU.
Gestational Diabetes: Managing Blood Sugar for Two
Gestational diabetes develops when your body can’t produce enough insulin to handle the increased blood sugar demands of pregnancy. It affects about 6-9% of pregnancies and is more common in women who are overweight, have a family history of diabetes, or are over 35.
The diagnosis usually comes after you fail the glucose tolerance test, which honestly sucks because that three-hour test is miserable. But once you’re diagnosed, the focus shifts to keeping your blood sugar levels stable.
First line treatment is always diet and exercise. You’ll meet with a nutritionist or diabetes educator who’ll teach you about counting carbohydrates and making food choices that keep your blood sugar from spiking.
The basic approach is eating smaller, more frequent meals throughout the day rather than three large meals. Pairing carbohydrates with protein helps slow sugar absorption. Choosing complex carbs like whole grains over simple sugars and refined carbs. Loading up on vegetables and lean proteins.
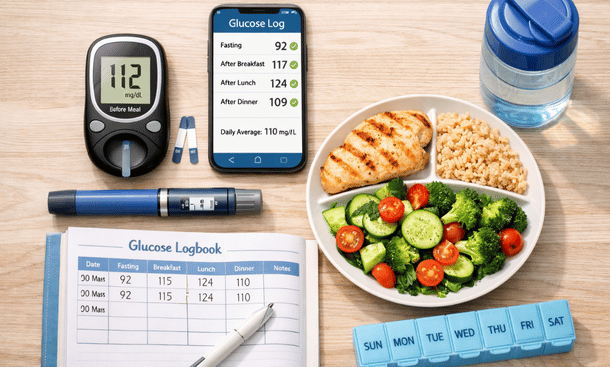
You’ll need to check your blood sugar multiple times a day with a glucose meter. Usually fasting when you wake up and then one or two hours after each meal. Your doctor will give you target ranges, typically under 95 fasting and under 120-140 after meals depending on their protocol.
Keeping a food and blood sugar log helps you identify which foods cause spikes and which ones keep you stable. You learn pretty quick that a bowl of pasta sends your numbers through the roof but a burger without the bun keeps you in range.
Exercise helps tremendously. Even just a 15-minute walk after meals can make a big difference in your blood sugar levels. Your muscles use glucose for energy, which helps bring those numbers down.
For many women, diet and exercise are enough to manage gestational diabetes through the rest of pregnancy. But somewhere around 10-20% need medication because lifestyle changes alone aren’t cutting it.
Insulin is the most common medication. It doesn’t cross the placenta so it’s safe for your baby. You’ll inject it before meals or at bedtime depending on when your numbers are running high. The idea of giving yourself shots is intimidating at first but you get used to it fast.
Some doctors use oral medications like metformin or glyburide instead of or in addition to insulin. These can be effective though there’s less long-term data on their use in pregnancy.
The concern with gestational diabetes is that high blood sugar can cause your baby to grow too large, which makes delivery more complicated and increases the risk of C-section. It also raises the chances of your baby having low blood sugar after birth and developing type 2 diabetes later in life.
But with good management, most women with gestational diabetes have healthy babies. You’ll probably get extra ultrasounds to monitor the baby’s growth and non-stress tests in the third trimester to make sure everything is going well.
The good news is that gestational diabetes usually goes away after delivery. Though it does mean you’re at higher risk for developing type 2 diabetes later, so you’ll need to stay on top of your health long-term.
Placenta Previa and Placental Abruption
Placental complications are scary because they directly affect how your baby gets oxygen and nutrients.
Placenta previa happens when the placenta covers part or all of the cervix. It’s usually discovered on an ultrasound in the second trimester, and the main symptom is bright red bleeding without pain.
There are different degrees of previa. Complete previa means the placenta totally covers the cervical opening. Partial or marginal previa means it’s close to or partially covering the opening. Low-lying placenta means it’s near the cervix but not quite covering it.
The treatment for placenta previa depends on severity and how far along you are. Many cases diagnosed early in pregnancy resolve on their own as the uterus grows and the placenta moves away from the cervix. That’s why your doctor will do follow-up ultrasounds to see if it’s still there.
If you have previa and start bleeding, you’ll probably be put on pelvic rest, which means no sex, nothing in the vagina, no heavy lifting or strenuous exercise. Basically taking it easy to avoid triggering more bleeding.
Severe bleeding might mean hospitalization and bed rest. If the bleeding is life-threatening or if you’re close enough to term, emergency C-section might be necessary.
The big issue with previa is that you can’t deliver vaginally if the placenta is still covering the cervix at the end of pregnancy. You’ll have a scheduled C-section, usually around 36-37 weeks before you go into labor on your own.
Placental abruption is different and more dangerous. This is when the placenta separates from the uterine wall before delivery, which can deprive your baby of oxygen and cause serious bleeding for you.
The classic symptoms are severe abdominal pain that doesn’t go away, a hard or tender uterus, and sometimes but not always vaginal bleeding. It can happen suddenly, often triggered by trauma like a car accident or fall, or it can develop more gradually.
Small abruptions might be managed with bed rest and close monitoring if you’re not close to term and the baby seems okay. But significant abruption usually means emergency delivery regardless of how far along you are because the risks to both you and your baby are too high.
I know someone whose placenta abrupted at 32 weeks. No warning, just sudden severe pain and bleeding. She had an emergency C-section within 30 minutes and both she and her baby survived, though her daughter spent six weeks in the NICU. It was terrifying but the quick action by her medical team saved both their lives.
Preterm Labor: When Your Baby Wants Out Too Soon
Preterm labor is regular contractions that cause your cervix to dilate before 37 weeks. It’s one of the most common complications in high-risk pregnancies.
Signs include regular contractions, lower back pain that comes and goes, pelvic pressure like the baby is pushing down, menstrual-like cramping, or increased vaginal discharge. If you’re having more than four contractions in an hour before you’re full term, you need to call your doctor.
The first thing they’ll do if you go in with suspected preterm labor is check your cervix to see if it’s dilating or thinning. They might do a fetal fibronectin test, which checks for a protein that’s released when labor is starting. They’ll monitor your contractions and the baby’s heart rate.
If you’re in early preterm labor and less than 34 weeks, the goal is to stop it if possible. Tocolytic medications can slow or stop contractions temporarily. Common ones include terbutaline, nifedipine, and magnesium sulfate.
These meds don’t work for everyone and they only buy time, usually 48 hours. But those 48 hours are crucial because that’s enough time to give you steroid injections to help your baby’s lungs mature faster.
Two shots of betamethasone 24 hours apart can dramatically improve outcomes for premature babies. It reduces the risk of respiratory distress syndrome, bleeding in the brain, and other complications of prematurity.
Bed rest is often prescribed for preterm labor, though the evidence on its effectiveness is questionable. Still, many doctors recommend at least limiting activity and avoiding anything that might trigger contractions.
If your cervix is shortening or you’ve had preterm labor before, you might get progesterone supplementation. This can be vaginal suppositories or weekly injections starting in the second trimester. Progesterone helps keep the uterus quiet and can reduce preterm birth risk.
Cervical cerclage is a surgical option if you have cervical insufficiency, meaning your cervix starts opening too early without contractions. They literally stitch your cervix closed and remove the stitch around 36-37 weeks. It’s usually done between 12-14 weeks if you have a history of second trimester losses.
The hardest part about preterm labor is the uncertainty. Sometimes it stops on its own and you make it to term. Sometimes the meds work and buy you crucial extra weeks. Sometimes despite everything, your baby comes early.
Modern NICUs can do amazing things for premature babies. Survival rates for babies born at 28 weeks or later are over 90%. Even babies born at 24-26 weeks have decent survival chances, though they face more complications.

IUGR: When Your Baby Isn’t Growing Well
Intrauterine growth restriction means your baby is measuring smaller than expected for their gestational age. It’s different from just having a small baby. IUGR indicates the baby isn’t getting adequate nutrients or oxygen.
Causes include placental problems, maternal health conditions like high blood pressure or kidney disease, infections, chromosomal abnormalities, or unknown factors. Sometimes IUGR is detected on a routine ultrasound when measurements come back below the 10th percentile.
The approach to managing IUGR depends on the severity and what’s causing it.
First they’ll try to identify the cause through additional testing. Detailed ultrasounds to look at blood flow through the umbilical cord and to the baby’s organs. Doppler studies show whether the placenta is functioning properly. Possible amniocentesis if there’s concern about genetic issues.
You’ll get frequent growth scans, probably every 2-4 weeks, to track whether your baby is still growing even if they’re small. What matters is continued growth, not just absolute size.
Non-stress tests and biophysical profiles monitor how your baby is tolerating the situation. As long as the baby is growing and tests look reassuring, you can usually continue the pregnancy with close surveillance.
Treatment focuses on addressing underlying causes if possible. Controlling your blood pressure if that’s the issue. Treating infections. Managing other health conditions optimally.
There’s not much you can do directly to make your baby grow bigger, which is frustrating. Some doctors recommend extra rest to improve blood flow to the uterus. Staying well-hydrated and well-nourished matters. But sometimes despite doing everything right, the baby just stays small.
The difficult decision comes when tests show the baby is no longer doing well inside. If blood flow patterns become abnormal or if the baby stops growing entirely, early delivery might be safer than continuing the pregnancy even if you’re preterm.
That’s a heartbreaking choice. Balancing the risks of prematurity against the risks of staying in an environment where the baby isn’t thriving. Your medical team will help you understand the specific risks and benefits for your situation.
Many babies with IUGR do catch up in growth after birth once they’re getting adequate nutrition directly. Others remain smaller but are otherwise healthy. The outcomes really depend on what caused the growth restriction and how severe it was.
Cervical Insufficiency: When Your Cervix Can’t Hold On
Cervical insufficiency, sometimes called incompetent cervix, is when your cervix starts opening too early in pregnancy without contractions or labor. It’s a leading cause of second trimester pregnancy loss.
Risk factors include previous cervical procedures like LEEP or cone biopsy, uterine abnormalities, previous preterm birth or second trimester loss, or carrying multiples. Sometimes there’s no obvious cause.
The tricky part is that cervical insufficiency is often only diagnosed after you’ve already lost a pregnancy. It’s hard to predict who will have problems before it happens.
If you have risk factors or a history of second trimester loss, your doctor will monitor your cervix closely with transvaginal ultrasounds starting around 16-20 weeks. They’re looking for cervical shortening or funneling, where the cervix starts opening from the inside.
Treatment options include cervical cerclage, which is stitching the cervix closed. This is usually done between 12-14 weeks and removed around 36-37 weeks before you go into labor. The stitch reinforces the cervix and helps it stay closed.
There are different types of cerclage. McDonald cerclage is the most common, where they place a purse-string stitch around the cervix. Shirodkar cerclage is placed higher and is harder to remove. Abdominal cerclage goes through the abdomen and is used when vaginal cerclage has failed or isn’t possible.
Progesterone supplementation is another option, either alone or combined with cerclage. Vaginal progesterone suppositories or weekly progesterone injections can help prevent cervical shortening.
Pessary is a silicone device inserted into the vagina to support the cervix. Some studies show it can reduce preterm birth risk in women with short cervix, though results are mixed.
Activity restriction is usually recommended. How strict depends on your specific situation, ranging from just avoiding heavy lifting and strenuous exercise to complete bed rest.
The psychological toll of cervical insufficiency is enormous, especially if you’ve lost pregnancies before. Every twinge makes you panic. You’re terrified to move. The constant monitoring and uncertainty are exhausting.
But plenty of women with cervical insufficiency carry to term with proper intervention. It requires close medical management and vigilance, but successful outcomes are definitely possible.
Bed Rest: When You’re Told to Stop Moving
Let’s talk about bed rest because it comes up with so many complications even though the medical evidence supporting it is pretty weak.
Doctors prescribe bed rest for everything from preterm labor to preeclampsia to placenta previa to IUGR. The theory is that lying down improves blood flow to the uterus and reduces stress on your body and the baby.
The reality is that studies haven’t shown bed rest actually prevents complications or improves outcomes for most conditions. But doctors still recommend it, partly out of an abundance of caution and partly because they don’t have better options.
Bed rest can mean different things. Modified bed rest might mean just limiting activity, avoiding exercise and heavy lifting, working from home, resting several times a day. Strict bed rest means staying in bed except to use the bathroom and maybe brief showers. Hospital bed rest is exactly what it sounds like.
The physical effects of prolonged bed rest aren’t great. Muscle loss, bone density loss, blood clots, difficulty sleeping, constipation, and deconditioning that makes recovery after delivery harder.
The mental and emotional effects can be even worse. Isolation, depression, anxiety, feeling useless and disconnected from normal life. Financial stress if you can’t work. Relationship strain. It’s really hard.
If you’re put on bed rest, ask your doctor exactly what’s allowed and what isn’t. Can you sit up? Can you work on a laptop? Can you take short walks? Get specific guidelines rather than vague “take it easy” advice.
Find ways to stay connected and occupied. Video calls with friends and family. Movies and TV. Reading. Online support groups for women on bed rest. Gentle upper body exercises if allowed. Anything to combat the boredom and isolation.
Accept help. Let people bring you meals, help with household tasks, keep you company. This is not the time to be stoic and independent.
Remember that bed rest is temporary. You’re doing this for your baby. That doesn’t make it easy, but it can help you get through the hard days.
Medication Safety During Complicated Pregnancies
Managing pregnancy complications often means taking medications, which brings up anxiety about whether they’re safe for your baby.
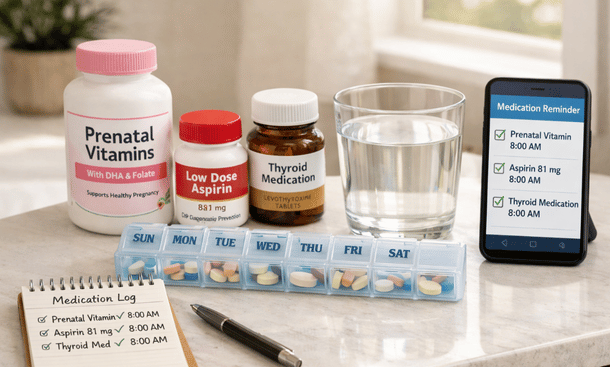
Low-dose aspirin is commonly prescribed for women at risk of preeclampsia. Studies show taking 81mg daily starting in the first trimester can reduce preeclampsia risk by about 15-20%. It’s considered very safe during pregnancy.
Blood pressure medications are necessary for chronic hypertension or preeclampsia. Labetalol and nifedipine are first-line choices during pregnancy. Some blood pressure meds aren’t safe, like ACE inhibitors and ARBs, so your doctor will switch you to pregnancy-safe alternatives.
Thyroid medications like levothyroxine are essential if you have hypothyroidism. Your dose often needs to increase during pregnancy, so regular blood work is important.
Insulin for diabetes is completely safe since it doesn’t cross the placenta. Same with metformin, which is increasingly used for gestational diabetes.
Blood thinners like heparin or Lovenox are necessary for women with clotting disorders or history of blood clots. These are safe during pregnancy, unlike warfarin which can cause birth defects.
Progesterone supplementation for preventing preterm labor or supporting early pregnancy is safe and widely used.
The key is weighing risks versus benefits. Untreated high blood pressure or uncontrolled diabetes or untreated clotting disorders are far more dangerous to your baby than the medications used to treat them.
Always tell your doctor about any supplements or over-the-counter medications you’re taking. Even things that seem harmless might interact with prescription medications or not be recommended during pregnancy.
Working with Maternal-Fetal Medicine Specialists
When complications arise, you’ll probably be referred to a maternal-fetal medicine specialist, also called a perinatologist. These are OB-GYNs with additional training in high-risk pregnancies.
The MFM doesn’t usually replace your regular OB. Instead, they work together to manage your care. Your OB handles routine prenatal visits while the MFM focuses on your specific complications and does specialized testing.
MFM appointments are typically longer and more detailed than regular OB visits. They do the detailed ultrasounds, interpret complex test results, and make recommendations about treatment plans.
Don’t be afraid to ask questions and advocate for yourself. These are the experts, but you know your body. If something doesn’t feel right or you don’t understand the plan, speak up.
Get copies of all your test results and reports. Keep them organized so you have the full picture of what’s happening. This is especially important if you end up seeing multiple specialists or going to the hospital.
Building a good relationship with your MFM team makes a huge difference. These are the people who will guide you through the scary parts and hopefully get you to a safe delivery.
Understanding how to manage complications is crucial, but so is taking care of yourself day-to-day while dealing with a high-risk pregnancy. Making smart lifestyle choices and practicing good self-care can improve your wellbeing even when medical challenges feel overwhelming.

Carlene R. Priddy offers strategic advice and practical guidance for governorsbefore, during, and after their mandatesto strengthen governance and public leadership.