
You saw that positive. Maybe it was faint, maybe it was clear as day. And then a few days later your period showed up anyway — heavier than usual, maybe with some cramping — and you were left holding a test wondering what just happened.
If that sounds familiar, there’s a real chance you experienced a chemical pregnancy. And the first thing I want you to hear is this: it was not something you did wrong.
I’ve been tracking my cycle for years. I’ve gone down the rabbit hole of hCG charts, implantation windows, luteal phase lengths — the whole thing. And when I first started researching chemical pregnancies, I was honestly surprised by how many people go through this without ever getting a real explanation of why. So let’s fix that.
What is actually happening during a chemical pregnancy
Before we get into causes, a quick grounding. A chemical pregnancy is a very early pregnancy loss — it happens around week four or five, usually before anything shows up on an ultrasound. The egg gets fertilized, implantation starts, your body produces enough hCG to trigger a positive test, and then the pregnancy doesn’t continue.
If you want to understand the full picture of what this experience looks like from start to finish, the complete breakdown of what a chemical pregnancy is covers everything in detail. Here we’re zooming in specifically on the why.
The main reasons a chemical pregnancy happens
Chromosomal abnormalities — the biggest one
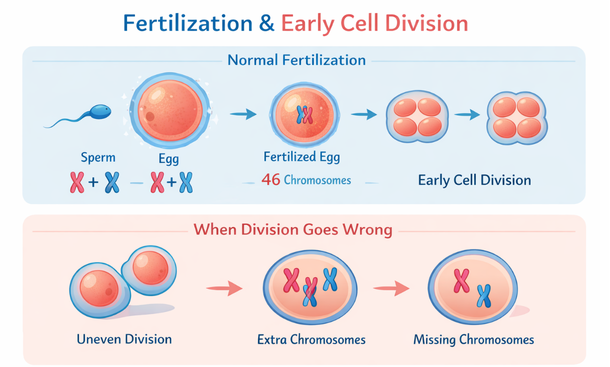
This is responsible for the majority of chemical pregnancies and honestly, early miscarriages in general. When an egg and sperm meet, their chromosomes combine. Sometimes that process doesn’t go perfectly — an error happens during cell division, or one of the reproductive cells had an abnormal chromosome count to begin with.
When the resulting embryo has chromosomal abnormalities, it usually can’t develop past a very early stage. The body recognizes something is off and the pregnancy doesn’t progress. This is not a reflection of your overall health or your fertility. It’s biology doing a quality check — harsh as that sounds.
The frequency of chromosomal issues increases slightly with age — particularly after 35 — but younger people experience this too. It’s one of those things that can happen to anyone, regardless of how healthy your lifestyle is.
Hormonal imbalances
Progesterone is essential in early pregnancy. It supports the uterine lining and creates the right environment for an embryo to implant and grow. If progesterone levels drop too early or are insufficient to begin with, the uterine lining can’t maintain itself — and the pregnancy ends.
Low progesterone is one of the more common hormonal causes of chemical pregnancies. Thyroid issues can also play a role. An underactive or overactive thyroid disrupts the hormonal balance that early pregnancy depends on. A lot of people don’t even know they have a thyroid issue until something like this prompts them to get tested.
If you’ve had more than one chemical pregnancy, asking your doctor about a progesterone check and a full thyroid panel is worth bringing up. It’s a simple blood draw and it can tell you a lot.
Uterine issues
The uterus needs to be in good shape for implantation to succeed. Some structural factors that can interfere with this include:
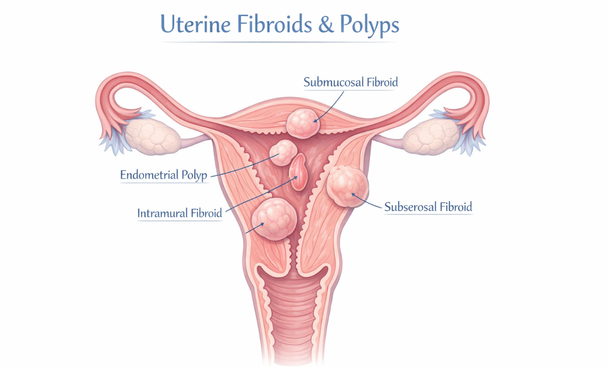
Uterine fibroids — noncancerous growths that, depending on their location, can block implantation or disrupt blood flow to the area where the embryo is trying to attach.
Uterine polyps — small tissue growths on the inner lining of the uterus that can make implantation difficult.
An abnormally shaped uterus — some people are born with a uterus that is septate, bicornuate, or otherwise structurally unusual. These variations can sometimes affect early pregnancy.
Most of these issues are diagnosable through ultrasound or a procedure called a hysteroscopy. And many are treatable if they’re found to be contributing to repeated losses.
Implantation failure
Sometimes the embryo itself is chromosomally normal and hormone levels are fine — but implantation just doesn’t take. The uterine lining may not be receptive at that particular moment. This can be related to timing, to the specific characteristics of the lining that cycle, or to factors that aren’t fully understood yet.
Reproductive medicine is still working out a lot of the details here. The honest answer is that implantation involves a complex conversation between the embryo and the uterine lining — and sometimes that conversation doesn’t connect.
Blood clotting disorders
This one is less common but worth knowing about. Conditions like antiphospholipid syndrome (APS) can cause the blood to clot abnormally. This can interfere with blood flow to the developing pregnancy and has been linked to early pregnancy loss.
If you’ve experienced recurrent chemical pregnancies — typically defined as two or more — your doctor may suggest testing for clotting disorders as part of a workup.
Infections
Certain infections, including some sexually transmitted infections, have been associated with early pregnancy loss when left untreated. This is less commonly the cause of a one-time chemical pregnancy, but it’s part of the picture.
Regular STI screening is something every person who is trying to conceive should have on their radar anyway — not because it’s likely to be an issue, but because it’s easy to rule out.
What does not cause a chemical pregnancy
This part matters. A lot of people go searching for something they did wrong — a workout, a glass of wine before they knew, stress, lifting something heavy. The research does not support these as causes of chemical pregnancy.

One chemical pregnancy does not mean something is fundamentally wrong with you. Most people who experience one go on to conceive and carry a healthy pregnancy without any intervention at all.
When to talk to a doctor
A single chemical pregnancy typically does not require medical investigation. But if you’ve had two or more, or if you’re tracking closely and noticing a pattern — that’s when it makes sense to loop in a reproductive endocrinologist or your OB.
They may suggest testing for hormonal issues, clotting disorders, uterine abnormalities, or chromosomal factors. Having that conversation early, especially if you’re actively trying to conceive, can save you a lot of time and emotional energy.
One more thing
Understanding why a chemical pregnancy happens is important. But it’s only one piece of what you’re going through. If you want to get into what the symptoms look like — how to recognize them in real time and understand what your body is doing — the next stop is chemical pregnancy symptoms: what to watch for.
That page breaks down the physical signs, the timeline, and how to tell the difference between a chemical pregnancy and a regular late period. If you’re tracking your cycle and want to know what the numbers and the bleeding are actually telling you, it’s worth the read.

As an author at Felyro.com, I create actionable content on pregnancy tracking, offering practical tools, tips, and insights that empower mothers-to-be to stay informed and confident throughout their pregnancy.