Okay, so you’re standing in the vitamin aisle trying to figure out which prenatal to buy, and you notice some say “folic acid” while others say “folate” or “methylfolate.” You’re probably thinking they’re the same thing, right? Different words for the same vitamin?
Yeah, that’s what I thought too. Turns out, we were both wrong.
And honestly, this isn’t just semantics or marketing nonsense. The difference between folic acid and folate actually affects how well your body can use this critical nutrient—and that has real implications for your baby’s development.
Let me break down what’s really going on here, why it matters for you specifically, and how to figure out which form you should be taking.
What Folate Actually Is
Folate is a B vitamin (B9, specifically) that exists naturally in foods. It’s the umbrella term for a whole group of compounds that your body needs for DNA synthesis, cell division, and red blood cell formation.
When you eat spinach, lentils, avocado, or other folate-rich foods, you’re getting natural folate in various forms. Your body takes these natural forms and converts them through several steps into the active form called 5-methyltetrahydrofolate, or 5-MTHF for short (because nobody wants to say that mouthful every time).
This active form—5-MTHF—is what your cells actually use. It’s the end product, the final destination, the form that does the heavy lifting in your body.
Think of it like this: natural folate from food is like raw ingredients that your body’s kitchen processes into the finished meal it can actually consume.
What Folic Acid Is (And Why It’s Different)
Folic acid, on the other hand, is the synthetic form of folate. It doesn’t exist in nature. Scientists created it in a lab, and it’s been the standard form used in supplements and food fortification since the 1990s.
Here’s the catch: folic acid isn’t biologically active. Your body can’t use it directly. It has to go through multiple conversion steps to become that same active 5-MTHF form.
For many women, this conversion process works just fine. Their bodies have the enzymes needed to transform folic acid into usable folate without any issues.
But for a huge chunk of the population—we’re talking 40 to 60 percent of people—this conversion process doesn’t work efficiently. And that’s where things get complicated.
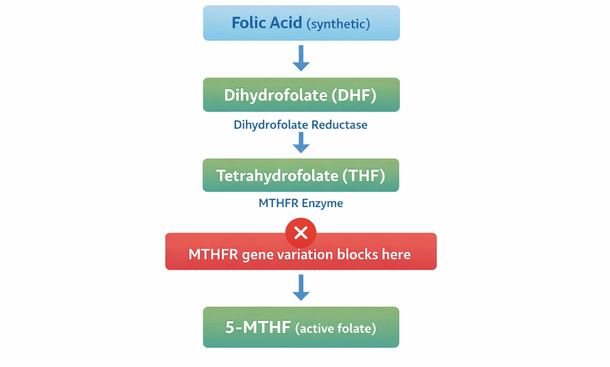
The MTHFR Gene Variation Nobody Warned You About
So here’s the science part, but I promise to keep it simple.
There’s a gene called MTHFR (methylenetetrahydrofolate reductase—yeah, it’s a nightmare to pronounce, which is why everyone just says the letters). This gene produces an enzyme that’s responsible for one of the key steps in converting folic acid into active folate.
About 40 to 60 percent of people have a variation in this gene that makes the enzyme less efficient. The two most common variations are called C677T and A1298C.
If you have one copy of the C677T variation (you’re heterozygous), your enzyme function drops to about 60 to 70 percent efficiency. If you have two copies (you’re homozygous), it can drop to 30 percent or lower.
What does this mean in real terms? It means that even if you’re taking folic acid supplements, your body might not be converting enough of it into the active form you actually need. You could be technically taking enough on paper, but functionally deficient in what your body can use.
And during those critical first weeks of pregnancy when the neural tube is forming? That’s a problem.
Why This Matters for Neural Tube Development
Neural tube defects like spina bifida and anencephaly occur when the neural tube doesn’t close properly in the first 28 days after conception. Adequate folate levels reduce this risk by up to 70 percent—but that’s assuming your body can actually use the folate you’re taking.
If you have an MTHFR variation and you’re only taking folic acid, you might not be getting adequate active folate to your developing baby during that crucial window. By the time you realize you’re pregnant, that window has often already passed.
This is why more and more doctors and fertility specialists are recommending methylfolate (the pre-activated form) instead of folic acid, especially for women who know they have MTHFR variations.
But here’s the thing: even if you don’t know your MTHFR status, taking methylfolate instead of folic acid doesn’t hurt. Your body can use it immediately without any conversion necessary. It’s like skipping all the middle steps and going straight to the finish line.
Folic Acid vs. Methylfolate: The Direct Comparison
Let me lay this out clearly so you can see the differences side by side.
Folic acid is synthetic, requires multiple conversion steps, doesn’t work efficiently for people with MTHFR variations, has been used in supplements since the 1990s, is cheaper to manufacture, and is still the form used in most prenatal vitamins and fortified foods.
Methylfolate (also called 5-MTHF or L-methylfolate) is the bioactive form, requires no conversion because it’s already in the form your body uses, works for everyone regardless of MTHFR status, has been available in supplements more recently, costs more to produce, and is increasingly found in premium prenatal vitamins.
The bottom line? Methylfolate is more universally effective. It works for everyone, while folic acid might leave a significant portion of women without adequate active folate levels.
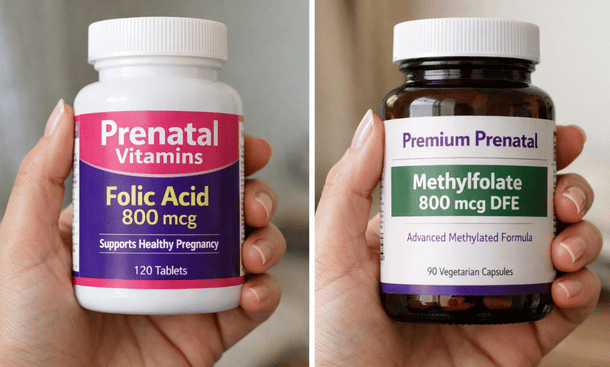
Prenatal Vitamins Comparison
Should You Get Tested for MTHFR?
This is a personal decision, and there are arguments on both sides.
Getting tested can give you definitive information about your genetic status. If you test positive for MTHFR variations, you’ll know for certain that methylfolate is the better choice for you. The test is usually a simple blood draw or cheek swab.
However, many doctors don’t routinely test for MTHFR variations, and insurance doesn’t always cover it. You can order direct-to-consumer genetic testing through companies like 23andMe, which includes MTHFR status in their health reports.
That said, here’s my take: whether you test or not, choosing methylfolate over folic acid is a safe bet that covers your bases either way. There’s no downside to taking the pre-activated form, even if you don’t have an MTHFR variation.
If you’re someone who likes having all the information before making decisions, get tested. If you’d rather just take the most effective form regardless, skip the test and go straight to methylfolate.
How Much Do You Need?
The recommended dose is the same whether you’re taking folic acid or methylfolate: 400 to 800 micrograms daily, starting at least one month before conception (three months is better).
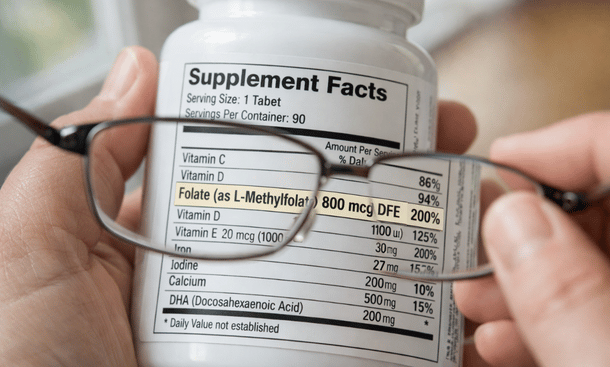
When you’re looking at supplement labels, you might see this listed as “mcg DFE” which stands for dietary folate equivalents. Don’t let that confuse you. For methylfolate, 400 mcg of methylfolate equals 400 mcg DFE.
For folic acid, the conversion is a bit different because it’s more bioavailable than food folate (ironically, even though it requires conversion, the synthetic form is actually absorbed better than natural food folate). So 400 mcg of folic acid equals about 667 mcg DFE.
Most prenatal vitamins contain 800 to 1,000 mcg DFE, which is perfectly safe and gives you a good buffer above the minimum recommendation.
What About Food Sources?
Here’s something important: when we talk about folic acid versus folate in supplements, that’s completely separate from the natural folate you get from food.
Food sources of folate—like dark leafy greens, lentils, beans, asparagus, avocado, and citrus fruits—provide natural folate that your body processes differently than synthetic folic acid. Eating these foods is always beneficial, regardless of your MTHFR status.
However, it’s really difficult to get the recommended 400 to 800 micrograms daily from food alone. You’d need to eat massive amounts of folate-rich foods every single day without fail. That’s why supplementation is recommended across the board for women trying to conceive.
One more note: in the United States, folic acid has been added to enriched grain products like bread, pasta, cereal, and rice since 1998 as a public health measure to reduce neural tube defects. This fortification program has been hugely successful, but it also means you’re getting folic acid whether you realize it or not if you eat these foods.
For women with MTHFR variations, this can contribute to unmetabolized folic acid circulating in the bloodstream, which some research suggests might not be ideal. This is another reason why choosing methylfolate in your supplement makes sense.
Reading Supplement Labels: What to Look For
When you’re shopping for prenatal vitamins, here’s how to tell what form of folate you’re getting.
If the label says “folic acid” or “folate as folic acid,” that’s the synthetic form.
If it says “folate as L-methylfolate,” “folate as 5-MTHF,” “folate as methylfolate,” or lists brand names like Quatrefolic or Metafolin, that’s the active form you want.
Some prenatal vitamins now use a combination of both forms. Personally, I’d prefer one that uses methylfolate exclusively, but a combination is still better than folic acid alone.
Also pay attention to the dose. You want at least 400 mcg, and 800 mcg is ideal. Some formulations go up to 1,000 mcg, which is also fine and safe for preconception.
The Cost Factor
Let’s be real: methylfolate supplements cost more than folic acid versions. That’s just the reality of the manufacturing process.
A basic prenatal with folic acid might run you ten to fifteen bucks a month. One with methylfolate could be twenty-five to forty dollars or more.
Is it worth it? I think so, especially if there’s any chance you have an MTHFR variation. You’re investing in the best possible start for your baby, and the cost difference works out to maybe fifty cents a day.
That said, I totally understand that budget matters. If the cost of methylfolate-based prenatals is genuinely prohibitive, taking folic acid is still way better than taking nothing at all. The fortification program has prevented thousands of neural tube defects using folic acid, so it clearly works for many women.
But if you can swing the extra cost, methylfolate gives you peace of mind that you’re covered regardless of your genetic makeup.
Other Nutrients That Work With Folate
Folate doesn’t work in isolation. It partners with other B vitamins, particularly B12, to do its job properly.
Vitamin B12 (cobalamin) works alongside folate in DNA synthesis and cell division. If you’re deficient in B12, you can have symptoms that look like folate deficiency, and high folate intake can actually mask a B12 deficiency.
This is especially important for women following vegetarian or vegan diets, since B12 is found almost exclusively in animal products. Make sure your prenatal contains adequate B12 (at least 2.4 micrograms), and consider getting your B12 levels tested before conception.
Vitamin B6 also plays a supporting role in the folate metabolic pathway. Most prenatal vitamins include B6, but it’s worth checking.
The point is, you want a well-rounded prenatal that covers all the essential nutrients we discuss in our breakdown of preconception nutrition, not just one that focuses solely on folate.
Making Your Decision
So what should you actually do with all this information?
If you know you have an MTHFR variation (either from previous testing or genetic reports), choose methylfolate without question. This is non-negotiable.
If you don’t know your MTHFR status but you have a family history of neural tube defects, have had previous pregnancy losses, or just want to be as cautious as possible, go with methylfolate.
If you’re on a tight budget and the cost difference is significant, folic acid is still a solid choice that has decades of research supporting its effectiveness. Just make sure you’re taking it consistently and starting at least a month before you try to conceive.
And if you’re somewhere in the middle—you can afford methylfolate but you’re wondering if it’s really necessary—I’d say go for it. The upside is significant, the downside is nonexistent, and you’ll have one less thing to worry about during an already stressful time.
Look, the whole folic acid versus folate thing might seem like splitting hairs, but when it comes to your baby’s neural development in those first critical weeks, getting this right matters.
The good news is that once you understand the difference, making the choice is actually pretty straightforward. Methylfolate works for everyone, bypasses the conversion issues that affect nearly half of all women, and gives you the confidence that your body is getting what it needs in a form it can actually use.
Now that you’ve got the folate piece figured out, the next step is knowing which prenatal vitamin actually delivers on quality and contains the right forms of all the nutrients you need. That’s where comparing your options becomes crucial—check out our guide to the best prenatal vitamins before pregnancy to see which brands are worth your money and which ones are just expensive marketing.
And don’t forget, this is just one piece of the preconception puzzle. Head back to our complete guide to preconception vitamins to make sure you’re covering all your bases before you start trying.