
So you’ve gotten your basic blood work done and everything checked out okay. Great! But if you’re over 35, dealin’ with irregular periods, or you’ve been tryin’ to conceive for a while without success, your doctor’s probably gonna suggest diggin’ a little deeper with hormone testing. And honestly? It’s a smart move.
Hormone tests give you concrete information about your fertility and reproductive health. They tell you whether you’re ovulatin’ regularly, how many eggs you’ve got left, and whether your body’s creatin’ the right environment for pregnancy. This isn’t about scarin’ you or makin’ you feel like you’re runnin’ out of time. It’s about givin’ you real data so you can make informed decisions.
Look, fertility can feel like this mysterious black box. You’re either pregnant or you’re not, and you don’t really know what’s happenin’ in between. Hormone testing opens that box and shows you what’s actually goin’ on inside your body. Knowledge is power, especially when it comes to somethin’ as important as startin’ a family.
Understanding Your Fertility Window
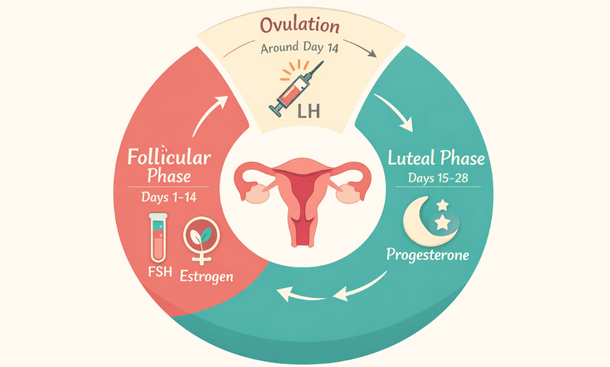
Before we dive into specific tests, let’s talk about what hormones actually do in your reproductive system. Your menstrual cycle is basically a carefully choreographed hormone dance. Different hormones rise and fall at different times, triggerin’ ovulation, thickenin’ your uterine lining, and either startin’ your period or supportin’ early pregnancy.
When these hormones are in balance, everything works smoothly. You ovulate regularly. Your periods come on schedule. Your body creates the perfect environment for an embryo to implant. But when hormones are outta whack, things can go sideways. You might not ovulate at all. Your periods might be irregular or absent. Or you might ovulate but not produce enough progesterone to support a pregnancy.
That’s where hormone testing comes in. These tests measure specific hormone levels at specific times in your cycle to see if everything’s functionin’ the way it should. The results can explain why you’re havin’ trouble gettin’ pregnant or help predict how much time you might have before your fertility starts to decline.
Anti-Müllerian Hormone: Your Ovarian Reserve Indicator
Let’s start with the big one. Anti-Müllerian hormone, or AMH, is probably the most talked-about fertility hormone these days. This test measures your ovarian reserve, which is basically how many eggs you’ve got left in the tank. Unlike some other hormone tests, AMH can be checked at any point in your cycle, which makes it super convenient.
Here’s how it works. Your ovaries contain tiny fluid-filled sacs called follicles, and each follicle contains an immature egg. The follicles produce AMH, so the more follicles you have, the higher your AMH level. As you age, your follicle count naturally decreases, and so does your AMH.
A higher AMH generally means you have more eggs available, which suggests better fertility potential. A lower AMH indicates a smaller egg supply. But here’s the thing. AMH tells you about quantity, not quality. You could have a low AMH but still get pregnant naturally if your eggs are healthy. Or you could have a high AMH but struggle with conception due to other factors like ovulation problems or egg quality issues.
Your doctor will interpret your AMH results based on your age. What’s considered normal for a 25-year-old is different from what’s normal for a 40-year-old. Generally speakin’, an AMH above 1.0 ng/mL is considered adequate for natural conception, but there’s a pretty wide range of normal. Some women with AMH levels below 1.0 still get pregnant without help, while others with higher levels need assistance.
If your AMH comes back low, don’t panic. It doesn’t mean you can’t get pregnant. It just means you might wanna move things along instead of waitin’ another year or two. Your doctor might recommend tryin’ to conceive sooner rather than later, or considerin’ fertility treatments if you’ve been unsuccessful after several months.
Follicle-Stimulating Hormone: The Ovulation Trigger
Follicle-stimulating hormone, or FSH, is another key player in your fertility story. Your pituitary gland releases FSH at the beginning of each menstrual cycle to stimulate your ovaries to grow follicles. As those follicles mature, they produce estrogen, which signals your pituitary to slow down FSH production.
FSH is typically measured on day three of your cycle, along with estrogen. This timing is important because it captures your baseline hormone levels before ovulation kicks in. High FSH levels on day three can indicate that your ovaries aren’t respondin’ well to the hormone signal. Basically, your pituitary is workin’ overtime to get your ovaries to do their job.
Elevated FSH often correlates with diminished ovarian reserve. When you have fewer eggs available, your ovaries produce less estrogen, so your pituitary pumps out more FSH to compensate. It’s like your body’s yellin’ louder to get a response. FSH levels above 10 mIU/mL are generally considered elevated, though some docs use different cutoffs.
Here’s what gets tricky. FSH can fluctuate from cycle to cycle. You might have a normal FSH one month and an elevated one the next. That’s why some doctors prefer to test FSH over multiple cycles or combine it with other tests like AMH to get a clearer picture. One elevated FSH doesn’t necessarily mean your fertility is doomed, but it’s definitely worth payin’ attention to.
Estradiol: Setting the Stage for Ovulation
Estradiol is the main form of estrogen in your body during your reproductive years. It’s produced by your ovarian follicles as they grow and mature. Estradiol does a bunch of important jobs. It thickens your uterine lining to prepare for potential implantation. It helps produce fertile cervical mucus that allows sperm to swim through. And it triggers the surge of luteinizing hormone that causes ovulation.
Like FSH, estradiol is usually measured on day three of your cycle. The test gives your doctor a baseline reading before your estrogen levels naturally rise as you approach ovulation. Normal day-three estradiol typically falls between 25 and 75 pg/mL, though ranges can vary by lab.
Low estradiol can indicate poor ovarian function or problems with follicle development. High estradiol on day three is actually more concernin’ than low levels. Elevated early estradiol might mean you have a dominant follicle that started growin’ from the previous cycle, which can throw off your hormone balance and interfere with normal follicle recruitment.
High day-three estradiol can also artificially suppress FSH levels, makin’ your FSH look normal even when your ovarian reserve is declining. That’s why your doctor will look at FSH and estradiol together rather than in isolation. If your FSH looks fine but your estradiol is high, it might be maskin’ an underlying fertility issue.
Luteinizing Hormone: The Ovulation Signal
Luteinizing hormone, or LH, is what actually triggers ovulation. About 24 to 36 hours before you ovulate, your LH level surges dramatically. This surge causes the dominant follicle to release its egg, startin’ the second half of your cycle. Home ovulation predictor kits work by detectin’ this LH surge in your urine.
Your doctor might check your baseline LH level on day three of your cycle along with FSH and estradiol. A normal LH-to-FSH ratio is usually around 1:1. But if your LH is significantly higher than your FSH, it could indicate polycystic ovary syndrome, or PCOS. Women with PCOS often have LH-to-FSH ratios of 2:1 or 3:1.
PCOS is one of the most common causes of infertility in women. It’s characterized by irregular ovulation, high androgen levels, and multiple small cysts on the ovaries. High LH is just one piece of the diagnostic puzzle, but it’s an important clue. If your LH is elevated, your doctor will probably run additional tests to check for PCOS.
Some doctors also use LH monitoring to time intercourse or insemination during fertility treatment. By trackin’ your LH surge, they can pinpoint exactly when you’re about to ovulate and maximize your chances of conception. This is especially helpful if your cycles are irregular or unpredictable.
Progesterone: The Pregnancy Support Hormone
Progesterone is sometimes called the pregnancy hormone because it plays a crucial role in supportin’ early pregnancy. After ovulation, the empty follicle transforms into something called the corpus luteum, which pumps out progesterone. This hormone thickens and enriches your uterine lining, creatin’ a nourishing environment for a fertilized egg to implant.
Progesterone is typically tested about seven days after ovulation, which is usually around day 21 of a 28-day cycle. If you have longer or shorter cycles, your doctor will adjust the timing accordingly. The goal is to check progesterone at its peak level during the luteal phase.
A progesterone level above 10 ng/mL generally confirms that you ovulated. Levels above 15 ng/mL suggest strong ovulation. Low progesterone in the luteal phase can make it hard to get pregnant or maintain a pregnancy. This condition, called luteal phase defect, means your body isn’t producin’ enough progesterone to support implantation.
If your progesterone comes back low, your doctor might prescribe progesterone supplements to use after ovulation. These can be pills, vaginal suppositories, or injections. The supplements help support your uterine lining and give an embryo a better chance of implanting successfully. Many women who experience recurrent miscarriages benefit from progesterone supplementation.

Thyroid Hormones and Prolactin
I know we already talked about thyroid testing in basic preconception blood work, but it’s worth mentionin’ again here because thyroid function directly affects your fertility hormones. Your thyroid-stimulating hormone, or TSH, should ideally be below 2.5 mIU/L when you’re tryin’ to conceive. Higher levels can interfere with ovulation and increase miscarriage risk.
Prolactin is another hormone that can throw off your fertility. This hormone is responsible for milk production after you have a baby, but it’s also present in small amounts when you’re not pregnant or breastfeedin’. High prolactin levels can suppress ovulation and cause irregular periods or even stop them completely.
Elevated prolactin, a condition called hyperprolactinemia, can be caused by certain medications, stress, thyroid problems, or a benign tumor on your pituitary gland called a prolactinoma. If your prolactin is high, your doctor will investigate the cause and treat it accordingly. The good news is that prolactin issues are usually very treatable with medication.
Some women don’t realize their prolactin is elevated because the symptoms are subtle. You might notice irregular periods, difficulty gettin’ pregnant, or occasional breast discharge even when you’re not pregnant or nursin’. If you have any of these symptoms, definitely mention them to your doctor so they can check your prolactin level.
Testosterone and DHEA-S: The Androgen Check
Androgens are typically thought of as male hormones, but women produce them too, just in smaller amounts. Testosterone and DHEA-S, or dehydroepiandrosterone sulfate, are the main androgens your doctor might test. Elevated androgen levels can indicate PCOS or other ovulation disorders.
High testosterone can cause symptoms like excess facial or body hair, acne, and scalp hair loss. It can also interfere with normal follicle development and ovulation. DHEA-S is produced by your adrenal glands, and elevated levels can suggest adrenal issues that might affect fertility.
If your androgens come back high, your doctor will likely run additional tests to diagnose PCOS or rule out other conditions. Treatment usually involves medications like metformin or letrozole to help regulate ovulation. Some women also benefit from oral contraceptives to lower androgen levels before tryin’ to conceive, though obviously you’d stop the pills when you’re ready to start tryin’.
The combination of high LH, high androgens, and irregular periods strongly suggests PCOS. But you don’t need to have all three to be diagnosed. PCOS is actually a spectrum disorder, and symptoms vary widely from woman to woman. Hormone testing helps your doctor figure out exactly what’s goin’ on so they can tailor treatment to your specific situation.
When to Get Hormone Testing
So when should you actually get these tests done? If you’re under 35 and you’ve been tryin’ to conceive for a year without success, it’s time to see a doctor and discuss hormone testing. If you’re over 35, don’t wait a full year. Six months of unsuccessful attempts is enough reason to get checked out.
You should also consider hormone testing sooner if you have irregular periods, very heavy or light periods, a history of pelvic inflammatory disease or endometriosis, painful periods, or symptoms of PCOS like excess hair growth or severe acne. Any of these issues can affect your fertility, and hormone testing can provide valuable insights.
Even if you’re not actively tryin’ yet but you’re in your mid-to-late 30s and thinkin’ about havin’ kids in the next few years, it’s not a bad idea to get baseline fertility testing. This is sometimes called fertility awareness testing or fertility MOT, like a car check-up. The information can help you make informed decisions about your timeline.
Fertility Test Reminder
Interpreting Your Results
Here’s the thing about hormone testing. The numbers don’t tell the whole story. You can’t just look at one result in isolation and draw conclusions. Your doctor needs to consider all your hormone levels together, along with your age, medical history, and symptoms, to get an accurate picture of your fertility.
For example, a 25-year-old with an AMH of 1.5 ng/mL and a 40-year-old with the same AMH are in very different situations. The younger woman’s result is concerningly low for her age, while the older woman’s result is pretty good. Context matters enormously.
Similarly, one abnormal result doesn’t necessarily mean you have a fertility problem. Hormones fluctuate. Stress, illness, diet, exercise, and sleep can all affect your levels. That’s why your doctor might repeat tests before drawin’ any major conclusions or recommendin’ treatment.
Don’t try to interpret your results on your own by googlin’ normal ranges. I know it’s tempting, but you’ll just drive yourself crazy. Different labs use different units of measurement and different reference ranges. What matters is how your doctor interprets your specific results in the context of your overall health and fertility goals.
What Happens If Something’s Off
If your hormone tests reveal an issue, your doctor will talk to you about next steps. Treatment depends on what the problem is. Low progesterone might be treated with supplements. PCOS might be managed with metformin or ovulation-inducing medications like Clomid or letrozole. Thyroid problems require thyroid medication.
Diminished ovarian reserve is trickier because you can’t increase your egg count. But that doesn’t mean you can’t get pregnant. Many women with low AMH or high FSH conceive naturally. Your doctor might recommend tryin’ for a few months and then considerin’ fertility treatment if needed. Time becomes more important when your ovarian reserve is limited, so you don’t wanna spend years tryin’ without success.
If your hormone issues are severe or you’ve been tryin’ for a while without success, your doctor might refer you to a reproductive endocrinologist. These are fertility specialists who can offer more advanced testing and treatment options like IUI or IVF. Don’t think of this as a failure. It’s just the next step in gettin’ the help you need.
The good news is that most hormone-related fertility issues are treatable. With the right diagnosis and treatment plan, many women go on to have successful pregnancies. The key is gettin’ tested, understandin’ your results, and workin’ with your doctor to address any problems.
Taking Control of Your Fertility Journey
Look, hormone testing can feel overwhelming. There’s a lot of information to process, and the results might bring up feelings of anxiety or stress. That’s completely normal. But try to remember that knowledge is empowering. These tests give you concrete information you can act on.
If your results are reassuring, you can relax a bit and keep tryin’ without worryin’ that somethin’s secretly wrong. If they reveal an issue, you can start treatment right away instead of wastin’ more time. Either way, you’re takin’ an active role in your fertility and makin’ informed decisions about your reproductive health.
Don’t be afraid to ask your doctor questions. If you don’t understand what a test measures or what your results mean, speak up. A good doctor will take the time to explain things in plain English and make sure you understand your options. If your doctor seems dismissive or rushed, consider gettin’ a second opinion. This is your body and your future family. You deserve clear answers and compassionate care.
Hormone testing before pregnancy gives you valuable insights into your reproductive health and fertility potential. Whether you’re checkin’ your ovarian reserve, confirmin’ that you’re ovulatin’, or investigatin’ irregular cycles, these tests provide concrete data that can guide your conception journey.
Remember that hormone testing is just one piece of comprehensive preconception planning. You’ve already completed your basic preconception blood work and genetic screening, which gave you a solid foundation. Now you’ve got a deeper understandin’ of your fertility hormones and reproductive function.
As you move forward with your preconception planning, don’t forget about the importance of STI screening and immunity tests before pregnancy. These screenings protect both you and your future baby from preventable infections that could affect fetal development.
For a complete overview of all the medical assessments you should consider before gettin’ pregnant, including hormone testing, blood work, immunity screenings, and partner testing, revisit our complete guide to preconception health tests. It brings together all the essential information you need to prepare your body for a healthy pregnancy.