So you just had your ultrasound and now you’re sitting there with this report that might as well be written in ancient Greek. Between the alphabet soup of abbreviations, numbers that mean nothing to you, and grainy black and white images where you can barely make out what’s supposed to be your baby, it’s enough to make anyone’s head spin.
I remember my first ultrasound like it was yesterday. The tech was moving that wand around my belly, clicking buttons, taking measurements, and I’m lying there thinking “just tell me if everything’s okay.” She hands me this printout covered in medical shorthand – CRL, BPD, HC, FL – and I’m nodding like I understand while secretly planning to spend the next three hours on Google trying to decode it all.
Here’s the thing though. Understanding your ultrasound results doesn’t require a medical degree. Once you know what those measurements mean, what the images are actually showing you, and what’s considered normal for each stage of pregnancy, the whole experience becomes way less stressful and way more meaningful.
You deserve to understand what’s happening with your baby at every appointment. Not just the “everything looks good” summary, but the actual details of how your baby’s growing and developing. So let me walk you through everything you need to know about pregnancy ultrasound results, from those first early scans all the way through to your anatomy scan and beyond.
Decoding ultrasound measurements and abbreviations
The first time you see an ultrasound report, it looks like someone just mashed their keyboard and threw in some random numbers. But those abbreviations actually tell you specific things about your baby’s growth and development.
Let’s start with the basics. Every measurement your sonographer takes corresponds to a specific part of your baby’s anatomy, and comparing those measurements to standardized growth charts helps your doctor track whether everything’s developing on schedule.
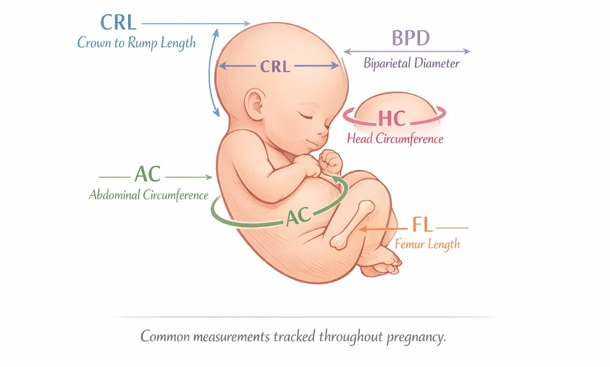
Crown-rump length, or CRL, is usually the first measurement you’ll encounter. This one’s pretty straightforward – it measures your baby from the top of their head down to their bottom. Your doctor uses CRL primarily in the first trimester, usually between 7 and 13 weeks, because it’s the most accurate way to date your pregnancy early on. Way more accurate than trying to remember the first day of your last period, especially if your cycles are irregular.
The measurement can pin down your due date within just a few days. At 8 weeks, normal CRL is around 1.6 cm. By 12 weeks, it’s usually around 5.4 cm. After about 14 weeks though, babies start curling up and stretching out at different times, which makes CRL less reliable for dating purposes.
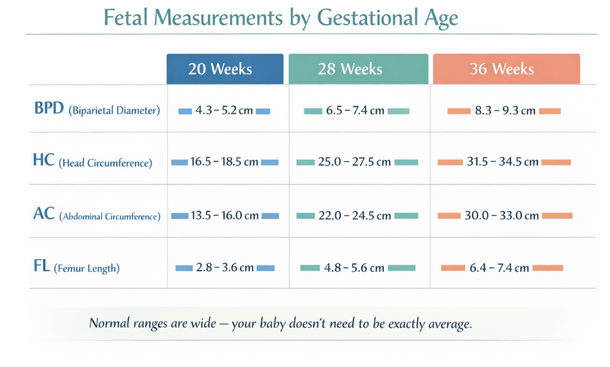
Biparietal diameter – BPD for short – measures the width of your baby’s head from one side to the other. Specifically, it’s measuring the widest part of the skull, right across those parietal bones. This measurement becomes important in the second and third trimesters and helps estimate your baby’s weight. It also confirms that their head is growing proportionally with the rest of their body.
Normal BPD measurements vary by gestational age, but generally speaking, at 20 weeks it’s around 4.7 cm and by 40 weeks it’s closer to 9.5 cm. Your doctor’s looking for steady growth rather than one perfect number. BPD is also one of the key measurements doctors use when they’re trying to figure out if you can deliver vaginally or if you might need a C-section.
Head circumference, or HC, goes all the way around your baby’s head instead of just across it. Think of it like measuring your waist versus measuring your width from side to side – both tell you something different. HC helps your doctor assess brain growth and development. If this measurement is tracking smaller or larger than expected, it doesn’t automatically mean something’s wrong. Some babies just have bigger or smaller heads, just like adults do. But significant deviations from the normal range might prompt your doctor to take a closer look.
Abdominal circumference – AC – measures around your baby’s belly at the widest point. The sonographer’s looking at the area where the stomach and liver are located, which gives them good insight into your baby’s overall nutrition and growth. AC is super important because it’s one of the main indicators of your baby’s weight.
If the AC is measuring small, your doctor might want to monitor more closely to make sure your baby’s getting enough nutrients through the placenta. If it’s measuring large, they might check for gestational diabetes. Here’s something that freaked me out the first time – AC measurements can vary quite a bit from one ultrasound to the next, even just a week or two apart. That’s because it depends partly on whether your baby just swallowed amniotic fluid or if they’re in a curled up position versus stretched out.
Femur length, or FL, measures the longest bone in your baby’s body – the thigh bone. It’s one of the easiest bones to measure clearly on an ultrasound because it shows up nice and bright on the screen. FL helps estimate gestational age and predicted birth weight. It’s also used to make sure your baby’s limbs are growing proportionally with their body.
Like all measurements, there’s a normal range, and some variation is totally expected. My daughter’s FL was consistently on the shorter side throughout my pregnancy, and guess what? She came out perfectly healthy, just with shorter legs. By 20 weeks, average FL is around 3.4 cm, and by full term it’s typically between 7 and 8 cm.
Now let’s talk about what those percentiles actually mean, because this part confuses everyone at first. When your doctor says your baby’s head is in the 60th percentile, they’re saying that if you lined up 100 babies at the same gestational age, your baby’s head would be bigger than 60 of them and smaller than 40 of them. That’s it.
Anything between the 10th and 90th percentile is considered totally normal. Most of the time, all your baby’s measurements will hover around the same percentile range. If your baby’s consistently measuring in the 30th percentile for everything, that just means you’re probably having a smaller baby. Not a problem as long as everything’s proportional and growing steadily.
What doctors look for is consistency and appropriate growth over time. A baby measuring in the 40th percentile at one scan and then the 38th percentile at the next scan is fine – that’s basically the same. A baby who drops from the 60th to the 20th percentile between scans might need closer monitoring.
Using all these measurements together, the ultrasound machine calculates an estimated fetal weight, or EFW. I’m gonna be real with you – this number can be off by quite a bit, sometimes by a pound or more in either direction. The formula combines several measurements, but it’s still just an estimate based on averages.
Your baby’s actual body composition, the amount of amniotic fluid, your body type – all these things can affect the accuracy. I’ve heard so many stories of women being told they’re having a huge baby, only to deliver a totally average-sized kid. Or being told their baby’s small and then out comes this chunky little thing. So take the EFW with a grain of salt, especially toward the end of pregnancy when babies are packing on weight fast.
If you want to dive deeper into what each of these abbreviations means and how the numbers change throughout your pregnancy, understanding pregnancy ultrasound measurements can help you feel way more confident at your next appointment instead of just nodding along while your mind races.
Understanding different types of pregnancy ultrasounds
Not all pregnancy ultrasounds are created equal, and trust me, you’re gonna have more than one during these nine months. Each type serves a different purpose in monitoring your baby’s development, and knowing what to expect from each scan helps you prepare mentally and understand what your healthcare team is looking for.
Let’s start with the two basic approaches. Transabdominal ultrasound is what most people picture – you lie back, the tech squirts that cold gel all over your belly, and then moves a device called a transducer across your skin. The gel helps the sound waves travel from the transducer through your skin and into your uterus. You’ll need a moderately full bladder for most of these, especially early in pregnancy, because it pushes your uterus up and out of your pelvis for better imaging.
Transvaginal ultrasound uses a slender wand-shaped transducer that’s inserted into your vagina. I know, sounds weird if you’ve never had one, but it’s really not as uncomfortable as it sounds. In early pregnancy, your uterus is still tucked down in your pelvis, and a transvaginal probe can get way closer to the action. The images are clearer and more detailed, especially before about 10 or 11 weeks.
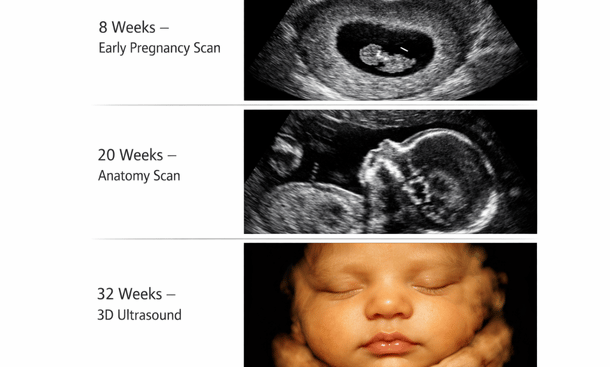
Your first official peek at your baby usually happens between 6 and 10 weeks with a viability or dating scan. The main goals are confirming that you’re actually pregnant, making sure the pregnancy is in the right place – in your uterus, not ectopic – seeing that heartbeat for the first time, and getting an accurate due date.
Most of the time this is done transvaginally because your baby is tiny. We’re talking the size of a blueberry or raspberry at this point. What you’ll see is pretty basic – a small gestational sac, a yolk sac that’s feeding your baby before the placenta takes over, and if you’re far enough along, a flickering heartbeat that’ll probably make you cry. I definitely did.
The first trimester screening, sometimes called the nuchal translucency or NT scan, happens toward the end of your first trimester between 11 and 14 weeks. It’s checking for chromosomal abnormalities like Down syndrome by measuring the fluid at the back of your baby’s neck. The NT measurement combined with blood work gives you a risk assessment, not a diagnosis.
At this scan, your baby actually looks like a baby for the first time instead of a blob. You might see them moving around, waving their little arms. It’s wild. They’ll also confirm your due date one more time and count fingers and toes if your baby cooperates with their positioning.
The anatomy scan around 18 to 22 weeks is the big one. This is the most detailed ultrasound of your pregnancy. Plan on being there for at least 30 to 45 minutes, sometimes longer if your baby’s being stubborn and won’t move into good positions.
The sonographer is checking everything – brain, spine, heart chambers and vessels, kidneys, bladder, stomach, all four limbs, the placenta, amniotic fluid levels, and your cervix. They’re taking tons of measurements and screenshots to make sure all your baby’s organs are forming correctly. This is also when most people find out the sex if they want to know.
Here’s something nobody tells you – sometimes they can’t see everything in one session. Maybe the baby’s curled up in a weird position or the placenta is blocking the view of something. Don’t freak out if they ask you to come back in a week or two for a follow-up. It’s super common and usually everything turns out fine once they get a better angle.
Some women get additional growth scans in the second or third trimester to check on baby’s size. This isn’t routine for everyone – it’s usually recommended if you have certain risk factors like gestational diabetes, high blood pressure, or if your baby was measuring small or large at the anatomy scan. These scans measure your baby’s head, abdomen, and femur to estimate their weight and make sure they’re growing appropriately.
If you make it to or past your due date, or if your doctor has any concerns about your baby’s wellbeing late in pregnancy, you might get a biophysical profile or BPP. This combines an ultrasound with a non-stress test. The ultrasound portion checks four things – fetal breathing movements, body movements, tone like flexing and extending, and amniotic fluid volume. Each component gets a score of either 0 or 2, and they add them all up.
Toward the end of pregnancy, around 36 weeks or so, your doctor might do a quick ultrasound just to confirm which way your baby’s positioned. Are they head down and ready to go, or are they breech with their butt or feet pointing toward your cervix? This scan takes like two minutes – they’re just confirming position so they can plan for delivery appropriately.
Now let’s talk about 3D and 4D ultrasounds. Regular ultrasounds give you 2D images – flat, black and white pictures. 3D ultrasounds use the same sound wave technology but the computer processes the data differently to create three-dimensional images of your baby’s face and body. 4D is basically 3D in real time, so you see a 3D video instead of still images.
Here’s the thing though – these aren’t typically part of routine prenatal care. They’re mostly done at specialty boutique ultrasound places, and you pay out of pocket. Some people love them and think they’re worth every penny. Others think they’re a waste of money when you’re gonna meet your baby face-to-face soon enough anyway. If you do want one, the best time is usually between 26 and 32 weeks.
Doppler ultrasound isn’t really a separate type of scan – it’s a technique that can be added to a regular ultrasound. Doppler measures blood flow through vessels, particularly the umbilical cord, the vessels in your baby’s brain, and sometimes the blood flow to your uterus. Your doctor might order this if there are concerns about your baby’s growth or if you have certain medical conditions.
Most low-risk pregnancies involve two or three ultrasounds total – one in the first trimester, the anatomy scan, and maybe one more toward the end. But certain situations mean you’ll be seeing that ultrasound machine a lot more often. Multiples pregnancies get way more monitoring. High-risk conditions require regular growth and position checks. IVF pregnancies typically get more early scans.
All these different scans can feel overwhelming when you’re trying to keep track of what’s happening when. But each one serves a specific purpose in monitoring your baby’s development and making sure everything’s progressing normally. The technology has come so far that we can catch and address issues early that would’ve gone undetected a generation ago.
If you want to know more about what happens at each specific scan and how to prepare for the different types of ultrasounds during pregnancy, that breakdown can help you understand exactly what your medical team is looking for at each stage and why certain scans use different approaches.
Reading and interpreting ultrasound images
Let’s be real for a second. You’re sitting in that ultrasound room, staring at the monitor, and all you see is what looks like a snowstorm with some random white blobs floating around. Meanwhile, the sonographer is going “oh look, there’s the nose” and you’re thinking “where? I don’t see anything that looks like a nose.”
Understanding what you’re actually looking at on that screen starts with knowing how ultrasound technology works. This isn’t like looking at a regular photograph where everything’s obvious. Ultrasound uses high-frequency sound waves that bounce off different tissues in your body.
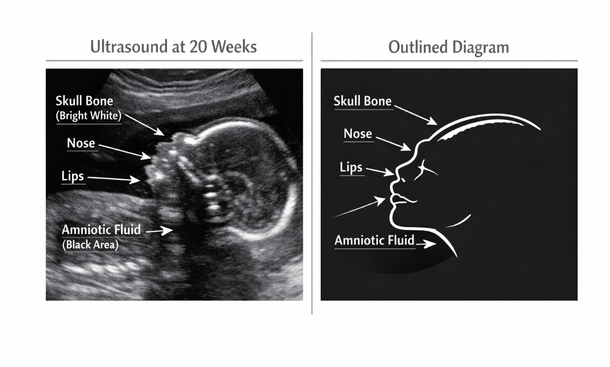
Dense tissues like bone reflect more sound waves back, so they appear bright white on the screen. Fluid doesn’t reflect sound waves much at all, so it shows up black. Everything else falls somewhere in between, creating those various shades of gray. That’s why your baby’s bones – skull, spine, limbs – show up as bright white lines and curves. The amniotic fluid surrounding your baby appears completely black. Your baby’s soft tissues like organs and muscle show up in different shades of gray depending on their density.
The black areas aren’t empty space, even though they look like it. That’s fluid, which is actually a good thing. You want to see that black around your baby – it’s the amniotic fluid keeping them cushioned and protected.
Early ultrasounds are the hardest to interpret because your baby is so tiny. At 6 or 7 weeks, we’re talking about something the size of a blueberry trying to show up on a screen. The first thing you’ll see is the gestational sac – a round or oval black circle. That’s the fluid-filled sac where your baby’s developing.
Inside that, you might see a smaller circle called the yolk sac, which looks like a little ring. The yolk sac is feeding your baby before the placenta takes over. Your actual baby shows up as a small white curve or blob inside the gestational sac. They call it the fetal pole at this stage, which is just a fancy way of saying “that’s your baby but they don’t look like much yet.”
The most exciting part of early ultrasounds is seeing the heartbeat. It shows up as a flickering or pulsing movement in that tiny fetal pole. On the screen, it might not look like much, but that little flicker is your baby’s heart beating away at like 150 beats per minute. By about 12 or 13 weeks, your baby actually starts looking human-shaped. You can usually see the head as a larger round area, and sometimes you can make out the body and limbs.
The profile view is usually the easiest angle to recognize because it actually looks like a baby. You’ll see the rounded curve of the forehead, the little nose, sometimes an open mouth, and the chin. Here’s the trick – look for the bright white line of the skull first. Follow that curve and you’ll find where the face should be.
The nose sticks out slightly from the face, and you might see the nasal bone as a small bright line. The lips sometimes show up as a slightly darker line. If your baby’s facing the transducer straight on, you might see both eye sockets as two dark circles, kind of like a skull. Don’t freak out – it’s just the angle and the fact that eye tissue doesn’t reflect ultrasound waves well.
Later in pregnancy, especially with 3D ultrasounds, you can sometimes see your baby’s expressions. They might look like they’re yawning, sucking their thumb, or making faces. It’s pretty wild when you catch them at the right moment.
The head is usually the easiest part to identify because it’s the biggest rounded structure you’ll see, and the skull shows up bright white. In the second and third trimesters, you can often see the brain structures inside the head as different shades of gray.
The spine is one of my favorite things to spot on ultrasounds because it’s so distinctive once you know what you’re looking for. It shows up as a row of bright white dots or dashes running down your baby’s back. Each little bright spot is a vertebra. Sometimes you see it from the side as a curved line, other times from behind as two parallel rows of dots.
The ribcage looks like a bunch of thin curved white lines surrounding the chest area. The body itself appears as various shades of gray. The organs inside – heart, stomach, bladder, kidneys – each have their own appearance. The stomach might show up as a small dark circle because it contains fluid. The bladder looks similar.
Limbs show up as long white bones with gray soft tissue around them. The femur is usually the easiest to see because it’s the longest and straightest bone. It looks like a bright white line. Arms are trickier because they’re smaller and babies tend to keep them bent up near their face.
Hands and feet are amazing when you can see them clearly. The individual finger bones and toe bones show up as tiny white lines. Sometimes you’ll catch your baby with their hand open, fingers spread, and you can count all five. Other times they’re in a fist. Feet often show up in profile, and you can see all the little toe bones lined up.
Don’t be surprised if you can’t see all the fingers and toes during your scan. Babies move constantly, and they’re often in positions where their hands and feet are hidden or curled up. The sonographer has ways to get better angles, but sometimes your baby just isn’t cooperating.
During your ultrasound, you’ll notice the sonographer keeps freezing the image and placing little crosses or plus signs on the screen. Those are measurement calipers, and they’re measuring various parts of your baby. When they measure the head, you’ll see the calipers go from one side of the skull to the other. For the abdomen, they measure around the belly. For the femur, they measure the length of the thigh bone from end to end.
The placenta usually shows up as a gray mass attached to the wall of your uterus. It might be at the top, bottom, front, or back. The texture looks kind of grainy or speckled. The umbilical cord shows up as a twisted rope-like structure connecting your baby to the placenta. With color Doppler, you can see blood flow through it – usually shown in red and blue colors on the screen.
Sometimes you’ll see the cord floating around in the amniotic fluid, and occasionally you might catch your baby holding onto it or playing with it. Babies actually do this a lot in utero.
You know how sometimes you see these perfect ultrasound pictures on social media where you can see every detail, and then your ultrasound looks like a blurry mess? Your baby’s position matters huge. If they’re facing the right direction with a good view of their face or body, the images will be clearer. If they’re facing your spine or curled up in a weird position, good luck getting a clear shot of anything.
How far along you are affects image quality too. The sweet spot for clear images is usually around 20 to 30 weeks. Early on, everything’s too small. Late in pregnancy, your baby’s too big and squished up. Your body composition plays a role. The amount of amniotic fluid matters. And honestly, the skill of the sonographer and the quality of the ultrasound machine make a difference.
If you’re struggling to identify what you’re seeing on the screen and want more help understanding how to read ultrasound pictures, that guide breaks down exactly what to look for and how to spot your baby’s features in those grainy images so you’re not just squinting and pretending you can see what the tech is pointing at.
Ultrasound Educational Comparison
Recognizing normal versus concerning findings
After every ultrasound, there’s that moment where you’re analyzing every word your doctor says, wondering if everything’s okay with your baby. Here’s the thing – what’s considered normal actually varies quite a bit depending on how far along you are and your unique pregnancy situation.
In the first trimester, normal means seeing a gestational sac in the right place – inside your uterus, not in a fallopian tube or anywhere else. The sac should be round or oval, with clear borders. By about 5 and a half to 6 weeks, you should see a yolk sac inside the gestational sac. This looks like a small ring and it’s feeding your baby before the placenta takes over.
The fetal pole should be visible by around 6 weeks, and the heartbeat – that’s the big one. By 6 to 7 weeks, you should see that little flicker of the heart beating. Normal heart rate in early pregnancy is between 110 and 170 beats per minute, though it’s usually on the higher end, like 150 to 170. If the heart rate is in this range and you can see a clear, strong flicker, that’s exactly what you want.
The nuchal translucency measurement, done between 11 and 14 weeks, should be less than 3 mm for most pregnancies. This measurement combined with blood work helps assess risk for certain chromosomal conditions. If it’s under 3 mm, that’s considered a reassuring finding.
At the anatomy scan around 20 weeks, there’s so much being measured and evaluated. For the head, a normal biparietal diameter at 20 weeks is around 4.7 cm, give or take. Head circumference should be around 17.5 cm. These measurements increase as pregnancy progresses, and there’s a range of normal for each week.
Abdominal circumference at 20 weeks is typically around 15 to 16 cm. This one can vary quite a bit based on whether your baby just swallowed some fluid or if they’re all curled up. Femur length at 20 weeks should be approximately 3.4 cm. Again, there’s normal variation here. Some babies have longer legs, some have shorter ones, just like adults.
The four-chamber view of the heart should show two atria and two ventricles that are roughly equal in size. The heart should be positioned on the left side of the chest and should be beating rhythmically. Normal fetal heart rate in the second and third trimesters is between 120 and 160 beats per minute.
Both kidneys should be visible and roughly the same size. You should be able to see the stomach as a small dark bubble in the abdomen – this shows your baby’s swallowing amniotic fluid. The bladder should also be visible as a dark circle in the pelvis. The spine should show all the vertebrae lined up with no gaps or protrusions. The skull should be completely closed with no openings.
The amount of fluid surrounding your baby is measured using different methods. One way is the amniotic fluid index, which adds up the deepest pockets of fluid in four quadrants of your uterus. Normal AFI is between 5 and 25 cm. Less than 5 is oligohydramnios, more than 25 is polyhydramnios.
Another method is the single deepest pocket. Normal is considered to be between 2 and 8 cm. Your fluid levels change throughout pregnancy. They increase until around 34 to 36 weeks and then start to decrease slightly toward your due date. This is totally normal.
The placenta can be positioned in different spots and still be totally normal. Fundal, anterior, posterior, or on either side – all of these are normal locations. What you don’t want is a placenta that’s covering your cervix, called placenta previa. Even if the placenta is low early in pregnancy, it usually moves up as your uterus grows.
Normal placenta thickness is roughly the same as the gestational age in millimeters until about 36 weeks. So at 20 weeks, around 20 mm thick is typical. The texture should look relatively uniform and smooth. The grade or maturity of the placenta increases as pregnancy progresses, and that’s normal.
Now let’s talk about some findings that sound scary when you first hear them but are actually pretty common and usually not concerning. Choroid plexus cysts are small fluid-filled spaces in the brain that show up on some second trimester ultrasounds. They’re present in about 1 to 2 percent of pregnancies and almost always go away on their own by the third trimester.
Echogenic intracardiac focus is a bright spot in the heart that shows up in about 5 percent of pregnancies. It’s usually just a normal variation in how calcium is deposited in the heart muscle. It doesn’t affect heart function and typically doesn’t mean anything is wrong.
Echogenic bowel means the baby’s intestines appear brighter than usual on ultrasound. This can be totally normal, or it can sometimes be associated with other conditions. If it’s the only finding and not severe, it’s often just a normal variant.
A two-vessel umbilical cord, missing one artery, occurs in less than 1 percent of pregnancies. Many babies with this are completely healthy, though your doctor might do some additional monitoring. Dilated renal pelvis, slight swelling in the kidney, is pretty common and often resolves on its own. Mild cases usually don’t cause any problems.
Sometimes your baby measures in the 70th percentile for head size but the 30th percentile for femur length. Before you panic, this is super common and usually not a problem. Babies, just like adults, have different body proportions. Maybe you have a tall family and your partner’s family is shorter. Your baby might have a longer torso and shorter legs – that’s genetics, not a problem.
What doctors look for is whether the measurements are roughly proportional. If the head is measuring way bigger than everything else, they might want to take a closer look. If the abdomen is measuring much smaller than the head and limbs, they might check placental function to make sure baby’s getting enough nutrition.
Small variations between percentiles are totally normal. We’re talking about differences of 20 or 30 percentile points being usually fine. It’s when you see major discrepancies that additional evaluation might be needed.
Appropriate growth means your baby is getting bigger over time at a steady rate. They should be following their own growth curve, even if that curve is at the lower or higher end of normal. In the second trimester, babies grow about 1.5 cm per week in length. Weight gain accelerates in the third trimester, with babies typically gaining about half a pound per week in the last month or so.
If your baby was measuring in the 40th percentile at 20 weeks and is still in the 35th to 45th percentile at 28 weeks, that’s good consistent growth. If they dropped from the 60th to the 20th percentile, your doctor would want to investigate why the growth slowed down.
Small for gestational age means measuring below the 10th percentile. Large for gestational age means above the 90th percentile. Both can be totally normal – some babies are just small or large – but they might warrant extra monitoring to make sure everything’s okay.
Sometimes you’ll get results that are technically within normal range but on the edge. Maybe your fluid is at 5.5 when normal is 5 to 25, or your baby’s measuring in the 12th percentile when normal starts at 10. Borderline doesn’t mean abnormal. It just means your doctor wants to keep a closer eye on things.
Usually the plan is just repeat ultrasounds in a week or two to make sure things aren’t getting worse. Sometimes they might recommend increasing your water intake, resting more, or making other small changes. Follow the monitoring schedule your doctor recommends and keep track of your baby’s movements.
Normal ultrasound results mean your baby is growing and developing the way they should be for their gestational age. It doesn’t mean every measurement is exactly at the 50th percentile or that everything looks identical to other babies at the same stage. Your baby is unique, and their measurements will reflect that.
As long as growth is consistent, measurements are roughly proportional, and your doctor isn’t expressing concerns, you can feel confident things are on track. Focus on the overall picture – is your baby growing, is the heart beating normally, are all the organs developing, is there good amniotic fluid? Those are the things that matter.
If you want to understand more about what specific findings are typical at each stage and when results might need follow-up, learning about normal ultrasound results in pregnancy can give you the reassurance you need instead of spending hours Googling and working yourself into a panic over numbers that are probably fine.
Questions to ask at your ultrasound appointments
You know that feeling when you walk out of your ultrasound appointment and suddenly remember all the questions you meant to ask? Or worse, you’re sitting there during the scan, watching the sonographer move that wand around, and you’re too nervous or overwhelmed to speak up even though you have no idea what’s happening?
Your ultrasound appointments are some of your best opportunities to get real information about how your baby’s developing. But you gotta know what to ask. Coming prepared with the right questions means you’ll actually understand what’s going on instead of leaving confused or worried.
Start with the basics about measurements and growth. Is my baby measuring on track for their gestational age? This is the big one. You want to know if your baby’s size matches up with how far along you are. Don’t just accept “everything looks good” – ask for specifics.
What percentile is my baby measuring in? Understanding whether your baby’s in the 30th percentile versus the 70th percentile helps you know if you’re having a smaller or larger baby. Remember, anywhere between 10th and 90th is normal.
Are all the measurements proportional to each other? Sometimes one measurement might be different from the others. You want to know if the head, abdomen, and limbs are all growing proportionally or if there are discrepancies that need monitoring.
How does this scan compare to my previous ultrasounds? Growth patterns matter more than single measurements. Is your baby following their own curve consistently? A baby measuring in the 40th percentile at one scan and then the 38th percentile at the next is fine – that’s basically the same.
What’s the estimated weight and how accurate is that estimate? Estimated fetal weight can be off by a pound or more, so it’s good to understand the margin of error. Don’t make major decisions based solely on weight estimates late in pregnancy.
During the anatomy scan especially, but really at any detailed ultrasound, you should ask about what they’re seeing. Can you show me the four chambers of the heart? The heart is complex and seeing all four chambers pumping normally is reassuring. Ask them to point out what they’re looking at.
Are both kidneys present and functioning? They should be able to see both kidneys and the bladder, which indicates the kidneys are producing urine. Is the brain developing normally? They check specific brain structures during the anatomy scan. Ask what they’re looking for and whether they saw everything they needed to see.
Is the spine completely closed? This checks for neural tube defects. They should be able to show you the vertebrae lined up with no gaps. Are all four limbs present with normal bone development? Make sure they counted all the fingers and toes, or at least tried to if your baby was cooperating.
Did you get good views of everything you needed to see? Sometimes the baby’s position makes it hard to see certain things. If they couldn’t see something clearly, ask when you should come back for a recheck.
The placenta is literally your baby’s life support system, so understanding how it’s functioning matters. Where is my placenta located? Knowing if it’s anterior, posterior, fundal, or low-lying helps you understand why you might or might not be feeling kicks strongly yet.
Is the placenta away from my cervix? If you have a low-lying placenta or placenta previa early on, ask if they expect it to move up as your uterus grows. Most do. Does the placenta look healthy and mature for this stage? The texture and grade of the placenta change throughout pregnancy.
Is blood flow to the placenta normal? If they did Doppler studies, ask about the results. Good blood flow means your baby’s getting adequate oxygen and nutrients.
Your amniotic fluid levels can tell you a lot about how things are going. Are my fluid levels normal? Get the actual measurement – whether it’s AFI or the deepest pocket measurement – and ask where it falls in the normal range.
If my fluid is low, what can I do about it? Sometimes increasing hydration helps with borderline low fluid. Ask if there are any steps you can take. If my fluid is high, what does that mean? High fluid can sometimes indicate gestational diabetes or other issues. Ask what they’re looking for and if you need additional testing.
Especially later in pregnancy, position matters for delivery planning. Which way is my baby facing right now? Early on this doesn’t matter much, but knowing if they’re head down, breech, or transverse later in pregnancy is important.
If my baby is breech, when should we talk about options? Most babies turn head-down by 34 to 36 weeks. If yours hasn’t, ask about external cephalic version or other options. Is there enough room for my baby to turn? Fluid levels and baby’s size affect whether they can still flip positions.
The cord connects your baby to the placenta, so its health matters. Does the umbilical cord have three vessels? Normal is two arteries and one vein. A two-vessel cord might warrant additional monitoring. Is blood flow through the cord normal? If they did Doppler ultrasound, ask about the resistance and flow patterns.
If the sonographer or doctor mentions any findings that seem concerning, here’s what to ask. What exactly did you find and what does it mean? Get them to explain in plain language, not just medical jargon.
Is this a common finding? Sometimes things that sound scary are actually present in a significant percentage of totally healthy pregnancies. What are the next steps? Do you need more testing, a follow-up ultrasound, consultation with a specialist?
What’s the best-case and worst-case scenario? Understanding the range of possibilities helps you prepare mentally without assuming the worst. How will this affect my pregnancy and delivery? Some findings require nothing more than extra monitoring. Others might change your birth plan.
Don’t be afraid to ask them to help you understand what you’re seeing on the screen. Can you show me where the baby’s head, body, and limbs are? Especially early on when everything looks like a blob, having them point things out helps tremendously.
What am I looking at when I see black areas? Understanding that black equals fluid helps you make sense of the image. Why does the baby look weird in this image? Sometimes the angle makes your baby look strange. Ask them to explain the view.
Can I get printed copies of the images? Most places give you a few printouts, but you can usually request more if you want them. Are you able to determine the sex? If you want to know and they haven’t mentioned it, go ahead and ask.
Make sure you understand the logistics too. When is my next ultrasound scheduled? Know the timeline before you leave. Why am I getting another ultrasound? Understanding the purpose helps you know what to expect and what they’ll be checking.
How soon should I hear from you about today’s results? Some results are available immediately, others need to be reviewed by your OB. Should I call if I notice anything concerning before my next appointment? Get clear guidance on warning signs to watch for.
Here’s how to actually get your questions answered without feeling rushed. Bring a written list of questions. Seriously, write them down before the appointment. You will forget otherwise. Prioritize your questions – put the most important ones first in case you run out of time.
Bring your partner or support person. Two sets of ears are better than one, especially when you’re emotional or overwhelmed. Take notes during the appointment or ask if you can record the conversation on your phone so you can review it later.
Don’t save all your questions for the very end. Ask as they go along when things are relevant. If the sonographer can’t answer medical questions, ask when you’ll speak with your doctor to discuss results. Sometimes techs aren’t allowed to interpret findings.
Look, some questions might feel dumb, but trust me, your doctor has heard them all before. Can you explain that again in simpler terms? If they used medical jargon you didn’t understand, make them break it down. Is this normal? Never be embarrassed to ask this. It’s your baby and your pregnancy.
Why are you measuring that? Understanding the purpose behind each measurement helps you learn what matters. How confident are you in these results? Ultrasound has limitations. Sometimes views aren’t clear or measurements can vary.
Your ultrasound appointments are opportunities to get valuable information about your baby’s health and development. Don’t waste them by being too nervous or embarrassed to speak up. Good doctors and sonographers want you to understand what’s happening. They’d rather spend a few extra minutes answering questions than have you leave confused or worried.
Come prepared, ask what you need to ask, and don’t leave until you understand the answers. This is your baby, your pregnancy, your body. You deserve to have all the information you need to feel confident and informed. And if you need help preparing your question list or want to know exactly what to ask about those measurements and abbreviations, checking out essential ultrasound questions to ask your doctor gives you a comprehensive guide to making the most of every appointment.

Understanding your pregnancy ultrasound results doesn’t have to feel like decoding some impossible puzzle. Those measurements, abbreviations, and grainy images all tell a story about how your baby’s growing and developing, and once you know what you’re looking at, the whole experience becomes way less stressful and way more meaningful.
Remember, those percentiles and numbers aren’t grades. Your baby doesn’t need to measure exactly average in every single category. What matters is consistent growth over time, measurements that are roughly proportional to each other, and a healthcare team that’s not expressing concerns about what they’re seeing.
The measurements – CRL, BPD, HC, AC, FL – each track a specific aspect of your baby’s development. The different types of ultrasounds serve different purposes throughout your nine months. Those black and white images show your baby’s bones as bright white, fluid as black, and soft tissues in shades of gray. Normal findings vary widely based on gestational age and individual variation. And asking the right questions helps you actually understand what’s happening at each appointment instead of just nodding along.
I spent way too many hours with my first pregnancy obsessing over every single number, comparing my baby’s measurements to online charts, convincing myself something was wrong because one measurement was a few millimeters off from “average.” Looking back, I wasted so much energy worrying about things that were completely fine.
What I wish I’d known then is that your doctor’s looking at the whole picture, not individual data points. They’re tracking trends, watching for proportional growth, making sure all the organs are developing properly. If they’re happy with how things are progressing, you can be too.
Trust the process, trust your medical team, and give yourself permission to actually enjoy these glimpses of your baby instead of turning every ultrasound into a source of anxiety. Your body knows what it’s doing, and modern ultrasound technology is just there to back it up and catch anything that needs attention.
Every pregnancy is unique, every baby grows at their own pace, and those ultrasound results are tools to help monitor development – not standards your baby needs to meet to pass some test. As long as growth is steady, measurements are proportional, and your doctor isn’t concerned, you’re doing great.
And look, if you’re still feeling overwhelmed or unsure about what you’re seeing on those reports, start by getting familiar with pregnancy ultrasound measurements explained so you can walk into your next appointment knowing exactly what those abbreviations mean and what numbers to pay attention to. Understanding the basics makes everything else fall into place.
Take a deep breath, ask your questions, trust your instincts, and remember that in just a few months you’ll be holding this little person in your arms instead of trying to make out their features on a fuzzy screen. Those ultrasound appointments are just snapshots along the journey, not the whole story.

As an author at Felyro.com, I create actionable content on pregnancy tracking, offering practical tools, tips, and insights that empower mothers-to-be to stay informed and confident throughout their pregnancy.