
Few things are more frustrating than a baby who just won’t latch onto your breast. You’re sitting there, breasts full of milk, baby crying and hungry, and no matter what you try, they either refuse to latch or latch so poorly that nobody’s happy. If you’re in this situation right now, especially in those early days or weeks, I want you to know you’re not failing and your baby isn’t broken.
Latching problems are incredibly common, and most of them have solutions once you figure out what’s actually going on. Sometimes it’s a physical issue with your baby’s mouth, sometimes it’s technique, sometimes it’s just a matter of patience and practice. We’re gonna walk through all the reasons babies struggle to latch and exactly what you can do about each one.
Why babies refuse the breast or can’t latch properly
Understanding the cause makes it way easier to fix the problem. There are a bunch of different reasons babies have trouble latching, and sometimes it’s a combination of factors.
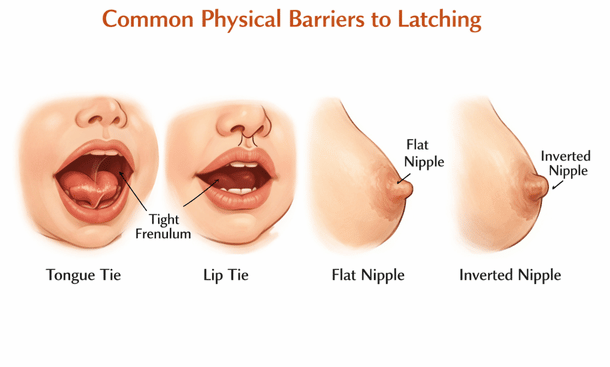
Tongue tie or lip tie are physical restrictions where the tissue under your baby’s tongue or upper lip is too tight. This prevents them from opening their mouth wide enough or moving their tongue properly to create a good latch. They might try to nurse but slip off repeatedly, make clicking sounds, or seem to work really hard without getting much milk. You might notice your baby can’t stick their tongue out past their bottom lip or their tongue looks heart-shaped when they cry.
Flat or inverted nipples make it harder for babies to latch because there’s less for them to grab onto. Your baby needs to take in a good amount of areola, not just nipple, and if your nipple doesn’t protrude much, they struggle to get a deep latch going.
Nipple confusion happens when babies get bottles or pacifiers early on and then prefer the different sucking motion or faster flow. They get frustrated at the breast because it requires more work and the milk doesn’t come as quickly.
Strong letdown or fast flow can overwhelm a baby, especially a newborn. If your milk comes out forcefully, your baby might pull off, sputter, cough, or refuse to latch because they can’t handle the spray.
Slow letdown or low supply creates the opposite problem. Your baby latches, sucks a few times, doesn’t get immediate reward, and gives up in frustration. They’re looking for instant gratification and aren’t patient enough to wait for letdown.
Positioning and technique issues are probably the most common cause of latching problems. If you’re not holding your baby at the right angle, not supporting their head properly, or not getting their mouth wide enough before they latch, it’s not gonna work well no matter how much you both try.
Pain from a previous difficult feeding can make babies develop an aversion. If latching hurt them before because of a bad latch or fast flow, they might remember that and resist trying again.
Nursing strikes can happen at any age where a baby who previously nursed fine suddenly refuses. These are usually temporary and triggered by things like teething, ear infections, changes in routine, or stress.
Prematurity or medical issues mean some babies just aren’t strong enough or coordinated enough to latch effectively yet. Their suck reflex might not be fully developed or they tire out too easily.
Techniques that help babies latch better
Let’s get into practical solutions you can try right now to help your baby latch successfully.
Skin-to-skin contact is magic for encouraging latching. Strip your baby down to just a diaper, take off your shirt and bra, and hold them against your bare chest. This triggers their feeding instincts and helps them naturally root and find the breast. Spend at least twenty to thirty minutes doing this before you even try to actively get them to latch.
Wait for a wide open mouth. This is crucial. Don’t try to shove your nipple into a partially open mouth. Tickle your baby’s lips with your nipple until they open really wide, like a yawn. Then bring them quickly onto your breast, aiming your nipple toward the roof of their mouth.
The C-hold or U-hold helps shape your breast and makes it easier for your baby to latch. Use your hand to compress your breast into a shape that matches your baby’s mouth. Keep your fingers well back from the areola so they’re not in the way.
Breast shaping or the nipple sandwich technique works great if you’ve got larger breasts or a smaller baby. Compress your breast from top and bottom so it’s flatter, like a sandwich, which makes it easier for your baby to get a big mouthful.
Express a little milk first to soften the areola if you’re engorged, and to give your baby an immediate taste of milk as motivation. Sometimes that little reward helps them stick with it.
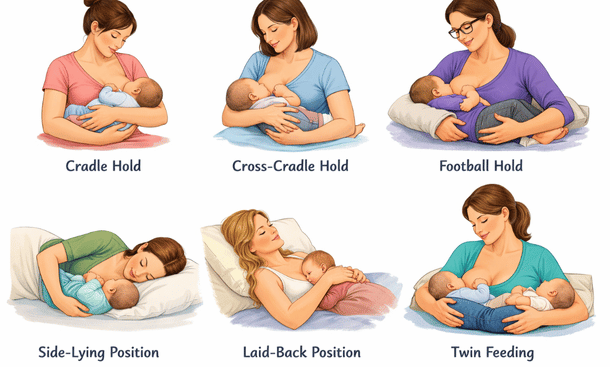
Try different nursing positions. The cross-cradle hold gives you the most control over your baby’s head and makes it easier to guide them onto the breast. The football hold works well if you’ve had a c-section or if your baby arches away in the cradle hold. Side-lying is good for relaxed, patient practice sessions. Laid-back or biological nursing positions let gravity help and allow your baby to use their natural reflexes.
The flipple technique helps get more breast tissue into your baby’s mouth. As your baby opens wide, use your finger to flip your nipple up toward their nose at the last second. This helps them scoop more of the bottom part of your areola into their mouth.
Pump or hand express to trigger letdown before latching if you’ve got a slow letdown. That way milk is already flowing when your baby latches and they get immediate reward.
If your flow is too fast, try laid-back positions where your baby is on top and gravity works with them instead of against them. You can also unlatch them when you feel letdown happening, let the initial spray go into a towel, then relatch once the flow calms down.
Dealing with tongue tie and lip tie
If you suspect a tongue or lip tie, you need to get it evaluated by someone who knows what they’re looking for. Not all pediatricians are trained to spot these, so you might need to see a lactation consultant, pediatric dentist, or ENT specialist.
A proper assessment involves looking at your baby’s mouth structure, watching them try to nurse, and evaluating how their tongue moves. They should check for a tight frenulum (that’s the piece of tissue under the tongue or upper lip) and see if it’s restricting movement.
If a tie is confirmed, the treatment is a simple procedure called a frenotomy or frenectomy. They clip or laser the restrictive tissue to release it. It takes literally seconds, causes minimal discomfort, and your baby can nurse immediately after.
Not all ties need to be released. If your baby is gaining weight fine and nursing isn’t painful for you, even a visible tie might not be causing functional problems. But if you’re dealing with poor weight gain, painful nursing, or your baby can’t maintain a latch, releasing the tie usually helps significantly.
After a tie release, you’ll need to do stretching exercises to prevent it from reattaching. Your provider will show you exactly what to do. You should also see improvement in latching within a few days, though sometimes it takes a week or two for your baby to figure out how to use their newly freed tongue.
Solutions for flat or inverted nipples
Flat or inverted nipples don’t make breastfeeding impossible, but they do require some extra strategies.
Nipple shields can be a helpful temporary tool. These are thin silicone covers that go over your nipple and give your baby something more prominent to latch onto. They’re not a long-term solution because they can reduce milk transfer, but they can get you through the early weeks while your baby gets stronger and your nipples get more elastic from nursing.
Nipple eversion techniques before nursing can help draw out flat nipples. Roll your nipple between your fingers, use a breast pump for a minute or two to pull it out, or use a syringe technique where you cut off the plunger end of a syringe, put the plunger in backward, and use the suction to draw out your nipple.

The good news is that nipples often become more protractile after a few weeks of nursing. Your baby’s sucking literally helps draw them out over time, so even if latching is hard at first, it usually gets easier.
Laid-back nursing positions work particularly well with flat nipples because your baby can use gravity and their instincts to compress breast tissue and draw the nipple into their mouth.
Overcoming nipple confusion and bottle preference
If your baby got bottles early on and now prefers them to breastfeeding, it takes patience and strategy to get them back to the breast.
Stop or minimize bottle use if possible. I know this isn’t always realistic, especially if you’re back at work or if supply issues mean you need to supplement. But the more bottles your baby gets, the stronger their preference becomes.
When you do give bottles, use paced bottle feeding. This means holding the bottle horizontal instead of tipped down, letting your baby control the flow by sucking rather than just letting milk pour into their mouth, and taking breaks during the feeding. This makes bottle feeding more similar to breastfeeding in terms of effort and pacing.
Start nursing sessions when your baby is calm and alert, not starving. A desperately hungry baby won’t have the patience to work at the breast when they know a bottle gives faster results.
Offer the breast frequently throughout the day, especially during drowsy times when your baby is less likely to protest. Many babies will latch better when they’re sleepy or just waking up.
Use a supplemental nursing system if you need to give bottles but want to encourage breastfeeding. These devices let you tube-feed your baby pumped milk or formula while they’re latched at your breast, so they get the practice and stimulation of nursing along with the supplemental feeding.
Stay patient and persistent. It can take days or even weeks to reverse a strong bottle preference, but many babies do come back to the breast with consistent gentle encouragement.
Managing nursing strikes
Nursing strikes are heartbreaking because your baby was nursing fine and suddenly won’t. But they’re almost always temporary.
Figure out if there’s a trigger. Did your baby recently have shots? Are they teething? Do they have an ear infection that makes lying on one side painful? Did you change your soap, perfume, or deodorant? Did something stressful happen? Identifying and addressing the cause helps.
Keep offering the breast without pressure. Don’t force it, but make the breast available frequently. Try offering when your baby is very sleepy or just waking up, in the bath, while walking around, in different positions and locations.
Maintain your supply by pumping while your baby isn’t nursing. You need to keep your breasts drained so your supply doesn’t tank during the strike.
Feed your baby your pumped milk by cup, syringe, or spoon rather than bottle if possible. This keeps them from developing a bottle preference on top of the strike.
Lots of skin-to-skin contact, carrying your baby, and physical closeness can help them want to nurse again. Sometimes co-bathing while offering the breast works when nothing else does.
Most nursing strikes last three to five days. Some resolve in a day, others take a week or two. Stay consistent and patient.
When you need professional help
Some latching problems require expert intervention. Don’t hesitate to reach out if you’re struggling.
See a lactation consultant if you’ve tried everything and your baby still won’t latch or if nursing is extremely painful despite trying different techniques. They can observe a full feeding, spot issues you’re missing, and give you personalized strategies.
Get your baby evaluated by a pediatrician if they’re not gaining weight, having fewer than six wet diapers a day after the first week, or seem constantly hungry and unsatisfied.
Consider seeing a pediatric dentist or ENT if you suspect tongue or lip tie. These specialists can diagnose ties that pediatricians or lactation consultants might miss.
If you’re dealing with postpartum depression or anxiety that’s being made worse by breastfeeding struggles, talk to your healthcare provider. Your mental health matters just as much as feeding your baby.
Join a breastfeeding support group, either in person or online. Sometimes just hearing that other moms have dealt with the same thing and gotten through it helps enormously.
The truth about latching struggles
Latching problems are frustrating as hell, especially when you’re exhausted, your baby is crying, and you feel like you’re failing at something that’s supposed to be natural. But struggling with latching doesn’t mean you’re doing it wrong or that breastfeeding isn’t gonna work for you.
Most latching issues improve with time, practice, and the right support. Babies get bigger and stronger, their mouths grow, they get more coordinated. What’s impossible at two days old often becomes easy at two weeks old.
Some babies are just more challenging than others. If you’ve got a baby with a tongue tie, or who’s premature, or who’s particularly strong-willed about their bottle preference, you’re playing on hard mode. That’s not your fault.
It’s okay to use tools like shields, supplemental nursing systems, or bottles if that’s what keeps your baby fed and you sane while you work through the latching issues. These aren’t failures, they’re solutions.
And it’s also okay to decide that exclusive breastfeeding isn’t worth the stress and to do a combination of nursing and formula, or to exclusively pump, or to switch to formula entirely. Fed is best, and your mental health matters.
If you’re dealing with painful, damaged nipples alongside latching problems, our guide on how to fix sore nipples while breastfeeding covers relief strategies and techniques to heal your skin while you work on improving the latch. For a complete overview of all the breastfeeding challenges you might face and practical solutions for each one, check out our comprehensive resource on common breastfeeding problems and how to solve them.

As a Felyro.com content author, I develop actionable content on breastfeeding, translating research-backed information into practical advice for mothers. My goal is to help families establish healthy feeding habits, improve maternal confidence, and support infant development.