
Let me be honest with you right up front. If you’re managing a high-risk pregnancy, you’re gonna spend more time in medical offices than you ever thought possible.
Between blood draws, ultrasounds, non-stress tests, and specialist appointments, it can start to feel like monitoring your pregnancy is a full-time job. I remember weeks where I had three different appointments and felt like I practically lived at my OB’s office.
But here’s the thing nobody tells you when you first get labeled high-risk. All those tests serve a real purpose. They’re not just covering the doctor’s liability or making money for the medical system. Each one gives your care team critical information about how you and your baby are doing.
Understanding what these tests actually are, why your doctor orders them, and what the results mean can transform the experience from scary and overwhelming to manageable. You stop feeling like a passive patient getting poked and prodded for mysterious reasons and start feeling like an active participant in your own care.
So let’s walk through the most common tests you’ll encounter during a high-risk pregnancy and what you should actually expect at each one.
First Trimester Screening and Genetic Testing
Most high-risk pregnancies start with extra genetic screening in the first trimester, especially if you’re over 35 or have a family history of genetic conditions.
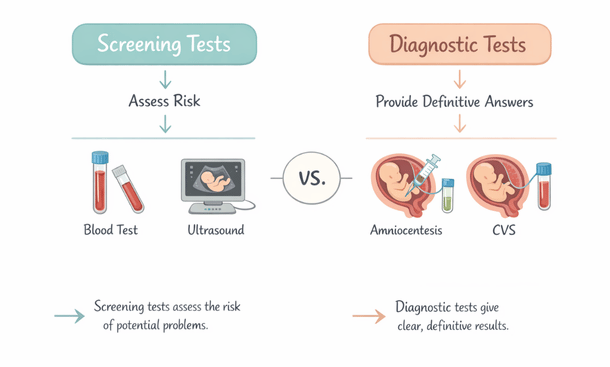
The first trimester combined screening usually happens between 11 and 14 weeks. It involves a blood test that measures two proteins in your blood and an ultrasound that measures the fluid at the back of your baby’s neck, called the nuchal translucency.
Together, these tests assess your risk for Down syndrome, trisomy 18, and some other chromosomal abnormalities. The results come back as odds, not definitive answers. Something like “1 in 10,000 chance” or “1 in 50 chance.”
If your results show increased risk, your doctor will probably recommend more definitive testing like CVS or amniocentesis. But the first trimester screen itself is completely non-invasive and poses zero risk to your baby.
Cell-free DNA testing, also called NIPT or non-invasive prenatal testing, is another option that’s become really popular. They just draw your blood and analyze tiny fragments of your baby’s DNA that are floating around in your bloodstream.
This test is more accurate than the combined screening and can tell you your baby’s sex super early if you want to know. It screens for the same chromosomal conditions plus a few others. Some versions can even detect certain genetic disorders.
The downside is that insurance doesn’t always cover it unless you’re considered high-risk or over 35. Out of pocket it can run several hundred dollars. But if you’re already in the high-risk category, you’ll probably get it covered.
CVS and Amniocentesis: When You Need Definitive Answers
These are the tests that freak people out because they involve actually taking a sample from inside your uterus.
Chorionic villus sampling, or CVS, happens earlier at 10-13 weeks. The doctor uses ultrasound guidance to insert a thin needle through your abdomen or sometimes through your cervix to collect a tiny sample of placental tissue.
That tissue has the same genetic makeup as your baby, so it can definitively diagnose chromosomal abnormalities and certain genetic disorders. The results usually take about two weeks, though some labs offer preliminary results sooner.
Amniocentesis happens later, typically between 15-20 weeks. This one involves inserting a needle through your abdomen into the amniotic sac to withdraw a small amount of amniotic fluid. The fluid contains cells from your baby that can be tested.
Both tests carry a small risk of miscarriage, usually quoted around 0.1-0.3%. That risk used to be higher, but doctors have gotten really good at these procedures with modern ultrasound guidance.
I’m not gonna lie, the idea of someone sticking a needle into my uterus terrified me. But the actual procedure wasn’t nearly as bad as I’d built it up in my head. There was some cramping during and after, kind of like period cramps, but it was over quickly.
You’ll need to take it easy for the rest of the day after either procedure. Most doctors recommend avoiding strenuous activity for 24-48 hours. You might have some light cramping or spotting, but heavy bleeding or severe pain means you need to call your doctor immediately.
The hard part is waiting for results. Those two weeks can feel eternal when you’re anxiously waiting to find out if your baby has a genetic condition. Try to stay busy and lean on your support system during that time.
Ultrasounds on Ultrasounds on Ultrasounds
Get ready to become very familiar with the ultrasound room if you haven’t already.
In a normal pregnancy, you typically get two or maybe three ultrasounds total. In a high-risk pregnancy, you might get one every few weeks or even weekly depending on what’s being monitored.
The anatomy scan around 18-22 weeks is standard for everyone. This is the detailed ultrasound where they check all of your baby’s organs and structures to make sure everything is developing normally. They measure the baby’s head, abdomen, and femur length. They check the heart chambers, kidneys, brain, spine, and all the other major systems.
For high-risk pregnancies, you’ll probably get additional anatomy scans or targeted ultrasounds focusing on specific concerns. If you have diabetes, they’ll monitor your baby’s growth closely because diabetic mothers tend to have larger babies. If you have high blood pressure or placental issues, they’ll check blood flow through the umbilical cord.
Growth scans later in pregnancy track whether your baby is growing appropriately. Babies that are too small (intrauterine growth restriction) or too large (macrosomia) both come with risks. The measurements help your doctor decide if and when intervention might be needed.
The biophysical profile is a specialized ultrasound that assesses your baby’s wellbeing by looking at movement, muscle tone, breathing practice, and amniotic fluid levels. Combined with a non-stress test, it gives a comprehensive picture of how your baby is doing.
Some women love getting all the extra peeks at their baby. Others find the frequent ultrasounds stressful because you’re always worried they’ll find something wrong. Both reactions are completely normal.

Non-Stress Tests and Fetal Monitoring
Once you hit the third trimester, non-stress tests become a regular thing for many high-risk pregnancies.
The test is called “non-stress” because it doesn’t put any stress on the baby. You basically sit in a recliner for 20-40 minutes while they monitor your baby’s heart rate and any contractions you might be having.
They strap two monitors around your belly. One picks up the baby’s heartbeat and the other detects contractions. You get a little button to press every time you feel the baby move.
What they’re looking for is whether your baby’s heart rate increases when they move, which is a sign of a healthy, well-oxygenated baby. They want to see at least two accelerations in heart rate over a 20-minute period.
If your baby is sleeping during the test, they might try to wake them up with a little buzzer or by having you drink something cold. Sometimes you have to sit there longer because your baby is being stubborn and not moving enough.
A reactive non-stress test is good news. It means your baby is doing well. A non-reactive test doesn’t necessarily mean something is wrong, but it requires further evaluation, usually with a biophysical profile or possibly admission to the hospital for continuous monitoring.
I did non-stress tests twice a week for the last month of my pregnancy. It got tedious sitting there for an hour each time, but I also found it weirdly reassuring. Hearing that steady heartbeat and seeing those little accelerations when the baby moved made me feel connected and helped calm my anxiety between appointments.
Bring your phone, a book, or something to keep you occupied. Some offices have TVs. The time passes faster if you’re not just staring at the monitor the whole time.
Glucose Tolerance Testing
Every pregnant woman gets screened for gestational diabetes, but high-risk pregnancies often get tested earlier and sometimes more than once.
The initial screening is the one-hour glucose challenge test. You drink a super sweet glucose drink (it tastes like flat orange soda) and then they draw your blood an hour later to check your blood sugar level.
If you fail the one-hour test, you have to do the three-hour glucose tolerance test. This one is more involved and honestly kind of miserable.
You have to fast overnight, then they draw your blood to get a baseline. Then you drink an even sweeter glucose solution and they draw your blood at one hour, two hours, and three hours after.
You can’t eat anything during those three hours and you usually feel pretty crappy from all that sugar on an empty stomach. I felt nauseous and shaky. Some women throw up, which means they have to come back and do the whole thing over again.
If you fail the three-hour test, you’re diagnosed with gestational diabetes and you’ll need to monitor your blood sugar regularly, adjust your diet, and possibly take medication or insulin.
Even if you pass initially, women with certain risk factors might get tested again later in pregnancy. High-risk pregnancies, especially those with obesity, family history of diabetes, or previous gestational diabetes, often warrant repeat testing in the third trimester.

Routine Prenatal Checkup
Blood Pressure Monitoring and Urine Tests
If you’re at risk for preeclampsia, get ready for your blood pressure to be checked at every single appointment. And I mean every single one.
They’ll probably also check it multiple times during each visit. Once when you first arrive, then again after you’ve been sitting calmly for a few minutes. Sometimes they’ll have you switch arms or change positions if they get an unusually high reading.
Blood pressure of 140/90 or higher on two occasions at least four hours apart indicates hypertension. Readings of 160/110 or higher are considered severely elevated and might warrant immediate treatment.
You might be asked to monitor your blood pressure at home between appointments. If so, your doctor will give you specific instructions about when to check it and what numbers should prompt a call to the office.
Urine tests at every visit check for protein, which is another sign of preeclampsia. A little protein can be normal, but significant amounts are concerning.
If they’re worried about preeclampsia, they might order a 24-hour urine collection. This is exactly what it sounds like. You collect all your urine for 24 hours in a big jug they give you, keeping it in your fridge between bathroom trips. Then you bring it back to the lab.
It’s inconvenient and kind of gross, but it gives the most accurate measurement of protein levels. Random urine samples can be affected by hydration and other factors, but the 24-hour collection averages everything out.
Blood tests can also help diagnose preeclampsia by checking your liver enzymes, kidney function, and platelet count. If your doctor is concerned, they’ll probably order a whole panel of tests to get the complete picture.
Fetal Echocardiography
Not everyone needs this specialized ultrasound, but it’s common if you have diabetes, a family history of heart defects, or if something looked concerning on a routine ultrasound.
Fetal echocardiography is basically an ultrasound of your baby’s heart done by a specialist, usually a pediatric cardiologist. They look at the structure of the heart chambers, valves, and major vessels to check for congenital heart defects.
This test typically happens around 18-24 weeks when the heart is developed enough to see clearly but early enough that you still have options if a significant defect is found.
The appointment takes longer than a regular ultrasound, usually 45 minutes to an hour. The specialist needs detailed views of the heart from multiple angles, which requires patience and sometimes waiting for the baby to shift into a better position.
Congenital heart defects are the most common type of birth defect, affecting about 1% of babies. Many of them are minor and don’t require any treatment. Others are more serious but can be corrected with surgery after birth.
Getting this test doesn’t mean your doctor thinks something is wrong. It’s often just a precaution based on your risk factors. Try not to panic before you even go in for the test.
Specialized Blood Tests
Beyond the standard prenatal blood work, high-risk pregnancies often require additional blood tests to monitor specific conditions.
If you have a clotting disorder or history of blood clots, you’ll get regular tests to check your clotting factors and make sure any blood thinners you’re taking are at the right dose.
Thyroid function tests are important if you have thyroid disease. Your thyroid hormone needs change during pregnancy, and keeping levels optimal is crucial for your baby’s brain development.
Women with autoimmune conditions like lupus get regular blood work to monitor disease activity and check for antibodies that could affect the baby.
If you’re Rh-negative, you’ll get antibody screens to check whether you’re developing antibodies against Rh-positive blood. This matters if your baby is Rh-positive. You’ll get a RhoGAM shot around 28 weeks and again after delivery to prevent problems in future pregnancies.
Anemia screening is standard, but high-risk pregnancies often need more frequent checks. Your iron levels can drop quickly, and severe anemia can cause complications for both you and your baby.
Group B strep testing happens around 35-37 weeks for everyone. If you’re positive, you’ll need antibiotics during labor to protect your baby from infection. It’s not a big deal but it’s important information for your delivery team.
Amniocentesis for Fetal Lung Maturity
This is different from the genetic amniocentesis done earlier in pregnancy. If you might deliver prematurely, your doctor might do an amniocentesis to check whether your baby’s lungs are mature enough to breathe on their own.
This usually only happens if delivery before 39 weeks is being considered for medical reasons. Maybe you have severe preeclampsia and need to deliver early for your safety. Or maybe your baby isn’t growing well and would be better off outside the womb even though they’re premature.
The test checks the levels of certain substances in the amniotic fluid that indicate lung maturity. If the lungs aren’t quite ready and delivery can safely wait, your doctor might give you steroid injections to speed up lung development.
Two shots of betamethasone 24 hours apart can dramatically improve outcomes for premature babies by helping their lungs mature faster. It’s standard treatment when preterm delivery is likely.
How Often You’ll Actually See Your Specialist
The frequency of appointments and testing depends on your specific situation, but expect to be seen a lot more than women with uncomplicated pregnancies.
In the first trimester, you might be seen every 2-4 weeks. By the second trimester, appointments often increase to every 2 weeks. In the third trimester, weekly visits are common, and some women are seen twice a week for monitoring.
If you’re working with a maternal-fetal medicine specialist in addition to your regular OB, you’ll be bouncing between offices. The MFM typically handles detailed ultrasounds and coordinates your specialized care plan while your OB manages routine prenatal visits
Some women find this level of monitoring reassuring. Every appointment confirms that things are still okay. Others find it exhausting and anxiety-provoking. Every test becomes another opportunity to hear bad news.
Both reactions are valid. There’s no right way to feel about being monitored this closely.
What Those Test Results Actually Mean
Understanding your test results is crucial but medical terminology can make everything sound scarier than it is.
Percentiles on growth scans indicate where your baby falls compared to other babies at the same gestational age. The 50th percentile is average. Anywhere from the 10th to 90th percentile is generally considered normal.
Below the 10th percentile indicates your baby is small for gestational age, which might be concerning or might just mean you’re having a petite baby. Context matters. If the baby is consistently tracking at the 8th percentile and everything else looks good, that might be normal for your baby.
What’s more concerning is when the growth rate changes. A baby who drops from the 60th percentile to the 20th percentile over a few weeks warrants closer investigation.
AFI, or amniotic fluid index, measures the amount of fluid around your baby. Normal is roughly 5-25 cm. Too much fluid (polyhydramnios) or too little (oligohydramnios) both need evaluation.
BPP, or biophysical profile score, is out of 8 or 10 points depending on whether the non-stress test is included. Each component gets either 0 or 2 points. A score of 8-10 is reassuring. Scores of 6 or below require further action.
Don’t leave your appointments confused about results. Ask your doctor to explain what the numbers mean and whether they’re seeing anything concerning. Sometimes results that sound scary are actually totally fine in context.
Preparing for All These Appointments
Practical tips for surviving the constant medical appointments that come with high-risk pregnancy monitoring.
Keep a dedicated pregnancy binder or folder with all your test results, appointment summaries, and important phone numbers. You’ll be juggling multiple providers and it helps to have everything in one place.
Use a pregnancy app or calendar to track appointments. Set reminders because when you’re seeing multiple doctors multiple times a week, it’s easy to mix up dates and times.
Prepare questions before each appointment. Write them down because pregnancy brain is real and you will forget what you wanted to ask.
Bring snacks and water, especially for longer appointments like non-stress tests or detailed ultrasounds. You might be there a while.
Don’t be afraid to ask for the first or last appointment of the day if that works better with your schedule. Early appointments mean less waiting but you have to get up early. Late appointments mean you might wait longer but you can work a full day first.
If you’re working, talk to your employer about the reality of frequent medical appointments. Some jobs are more flexible than others, but you’re legally entitled to reasonable accommodations for pregnancy-related medical care.
Bring a support person to important appointments if you can. Having someone else there to ask questions and remember information is helpful, especially when you’re getting potentially stressful test results.
The Emotional Toll of Constant Testing
All this medical surveillance takes a mental and emotional toll that doesn’t get talked about enough.
Some women develop serious anxiety around appointments. You’re constantly waiting for the other shoe to drop, for someone to find something wrong. That’s exhausting and can affect your whole pregnancy experience.
Others become almost numb to it all. Appointments become routine and you stop connecting emotionally to the process. You’re just going through the motions.
Finding a therapist who specializes in pregnancy and maternal mental health can be really valuable. Many OB practices now screen for anxiety and depression and can provide referrals.
Online support groups for high-risk pregnancy can help you connect with other women who understand what you’re going through. Sometimes it helps just to vent to people who get it.
Remember that these tests and appointments exist to help you have the healthiest pregnancy possible. They’re not punishment or unnecessary medicalization. They’re tools that give your care team information to make good decisions.
Try to celebrate the good appointments and good test results instead of just moving immediately to worrying about the next one. Your baby had a great non-stress test? That’s genuinely good news worth acknowledging.
All these tests provide crucial information, but knowing what to do when results show complications is where the rubber meets the road. Understanding your treatment options helps you make informed decisions about your care.

Carlene R. Priddy offers strategic advice and practical guidance for governorsbefore, during, and after their mandatesto strengthen governance and public leadership.